
Our analysis focused on factors guided by the CFIR associated with the outer setting, inner setting, and characteristics of individuals. Understanding these determinants provided insights into the complexities of healthcare transition and served as the foundation for understanding how the proposed Transition Compass intervention could mitigate barriers in the transition process. The findings are presented in two sections: the determinants of transition and the proposed Transition Compass intervention. Key quotes are provided in Tables 1–6. A more comprehensive list of quotes organised by CFIR domains and sub domains is provided as supplementary table 1. Table 2 provides an overview of the demographic characteristics of our sample, including the self-reported conditions of the AYAs who participated in the study as well as departments represented by adult and paediatrician HCP participants highlighting the diversity of experiences represented.
We used a process mapping approach to codify the transition pathways across various paediatric healthcare departments, highlighting the complexity and variability resulting from the absence of standardised and consistent processes across locations, institutions, and between diseases (supplementary table 2). This, in addition to our qualitative analysis, helped us to identify factors determining the potential success of interventions supporting transition. Our themes are organised according to the process of healthcare transition, healthcare provider factors impacting transition, and AYA factors impacting healthcare transition.
The Process of Healthcare Transition
Participants reported that the timing of healthcare transition is variable across institutions, contributing to several challenges and inconsistencies in the care AYAs receive. They shared that some healthcare providers begin the transition process as early as age 15 or 16, while others wait until the AYA is 18 or older. They noted that transition timing can also be influenced by major life changes, such as moving and/or starting university, acknowledging that if the AYA is uncertain about their future plans and location, the ability of paediatric HCPs to refer them to appropriate adult HCPs becomes complicated.
There were mixed views on initiating transition conversations early. While many considered early discussions helpful, some families and AYAs were not ready to fully engage with the information. Despite this, there was a generally strong desire for advanced notice about the differences between paediatric and adult care, to facilitate better preparation and avoid AYAs and families being unaware of the transition until it was imminent. Participants reported that a lack of AYA preparedness led to confusion and gaps in care, as adult services were less structured and frequent, compared to the regular, coordinated appointments in paediatrics. Additionally, participants reported that paediatric HCPs sometimes lacked prior awareness that an AYA was due for transition, only recognising the need at what should be their final paediatric appointment. This lack of early awareness hindered their ability to adequately prepare AYAs and their families for transition. Suggestions for improvement included starting discussions by at least around age 16 or 17, potentially earlier for those living with multiple complex and chronic health conditions and/or disability, and providing information and resources to help AYAs understand and adapt to adult care. Additionally, participants noted that offering tours or programmes to introduce young people to adult healthcare facilities could reduce the intimidation and anxiety associated with the transition.
Frequently noted by participants was the gap between AYAs having their last appointment in paediatric services and their first appointment in adult services. Many described this gap as a ‘falling off a cliff’ model of transition and questioned who was responsible for providing care during this period. Many paediatric HCPs described offering interim care on an ad-hoc basis due to long waitlists and delays in the adult system. This gap was compounded by a lack of formal processes to inform paediatric HCP referrers that the AYA had been seen by adult services. This ‘no man’s land’ during the transition left AYAs vulnerable to falling through the cracks, being removed from waitlists, or otherwise unable to progress their care in adult services. AYAs reported gaps in care due to their age, as they were considered too old for paediatric services but too young and/or physically too small for adult equipment and services. Fragmentation was further exacerbated by multi-morbidity, as the timing of transfer to each adult specialist varied. Differences in team acceptance ages led to some aspects of care remaining under paediatric services while others were transferred to adult services.
Participants shared differing opinions on the effectiveness of specialist transition services, which are usually services embedded in paediatric hospitals that support young people transition to the adult health care system and are staffed by medical, nursing and/or allied health professionals. Paediatric HCPs often referred AYAs with complex healthcare needs, such as those requiring multiple specialists, to these services. However, their experiences with the usefulness of these services varied. Additionally, many AYAs who could benefit from specialist transition expertise did not meet the criteria and were therefore excluded from receiving this support.
Healthcare Provider Factors Impacting Healthcare Transition
Our process mapping activity (supplementary table 2) and interview data indicated transition success was often better supported when there were established relationships between paediatric and adult specialists. Some paediatric HCPs had well established relationships with adult HCPs, however some expressed a lack of awareness and/or availability of relevant adult HCPs, as well as no established processes to acquire this knowledge. Without knowledge of available and appropriate adult HCPs for referrals, paediatric HCPs found it challenging to effectively connect AYAs to suitable adult care. Given the rarity of many paediatric conditions, they are often treated at a central tertiary centre. However, when transitioned to adult care, participants reported that AYAs become dispersed/treated at local hospitals, and paediatric HCPs struggle to maintain networks across all adult teams statewide to facilitate appropriate local referral. HCPs described efforts to navigate these challenges, including establishing joint paediatric-adult clinics, clinicians with dual employment across the paediatric and adult hospitals, or paediatric and adult services offering a period of collaborative, overlapping care. However, these opportunities were often ad-hoc, driven by individual clinician initiatives and hindered by barriers such as lack of administrative support and clinic facilities, difficulty scheduling HCP diaries, cost, and lack of interest or time by some adult HCPs.
AYA participants raised concerns about the transfer of medical information during the transition process. Paediatric records were commonly maintained on different electronic systems than those used in adult settings, with adult HCPs unable to access them. Healthcare professionals frequently relied on brief handovers that lacked essential details such as previous imaging or comprehensive medical histories. This sometimes led to unnecessary repetition of medical investigations. Paediatric HCPs described varying practices regarding the completion of treatment summaries for transfer to adult HCPs. While some paediatric clinicians routinely prepared these summaries, others were inconsistent due to challenges such as lack of formalised processes, time constraints, or difficulty in summarising extensive care spanning up to 18 years. Some HCP participants highlighted the importance of better communication and documentation systems. They proposed solutions such as transition passports or comprehensive transition letters containing vital medical summaries and recommendations for future care, including the current and anticipated frequency of appointments. A facilitating factor for information transfer was having electronic medical systems that were accessible across both paediatric and adult services. Adult HCPs expressed a desire for information on the social supports of the AYA to understanding the best approach to their care.
One significant challenge AYAs and their families faced during healthcare transition was adjusting to the differences in the care environment and the nature of support provided. Participants highlighted a contrast in the level of personalisation and nurturing between paediatric and adult settings. Participants characterised paediatric care as having a comprehensive, wrap-around approach with a strong emphasis on personalised, centralised care, and multi-disciplinary team collaboration. Paediatric services were also commended for providing follow-up and support, particularly around missed appointments, aiming to streamline care through coordinated scheduling. AYAs described a shift from coordinated, multidisciplinary care in paediatrics to fragmented services in adulthood, where accessing support and specialist services became more difficult and bureaucratic. AYAs expressed feeling like “just another number” in the adult system rather than an individual with specific needs. Additionally, adult services did not follow up missed appointments, discharging patients who did not attend or reschedule. In such situations, AYAs would present to care through the emergency department (ED).
Participants highlighted numerous challenges related to the role and expectations of GPs in the transition process. With no direct equivalent to a paediatrician in adult healthcare, participants noted that the GP often becomes the mainstay for AYAs, who many acknowledged are not resourced appropriately to provide this care. Participants noted that many AYAs may not have a regular GP or an established relationship with a GP due to the predominant involvement of paediatricians in their earlier care. The variability in the level of experience, knowledge and availability of GPs exacerbated the issue, with some regions, particularly rural and remote areas, facing severe shortages and others dealing with GPs who lacked the knowledge, confidence, and experience to manage rare conditions, comorbidities, and other complexities associated with CMCs. Participants noted that continuity of care may be disrupted when patients see different GPs at a clinic, rather than a consistent GP. Furthermore, the limited time available in GP appointments was often described as insufficient to address the complexities of chronic conditions.
Adolescent and young adult factors impacting healthcare transition
Participants reported that AYAs living with complex medical conditions and/or experiencing psychosocial complexity found healthcare transition particularly challenging. This was compounded by a lack of sufficient resources, such as for AYAs living with neurodiversity, mental health conditions and/or experiencing mental ill-health. According to participants, access was particularly challenging for AYAs who did not meet criteria for disability funding support from the Australian government. Geographic disparities further complicated access to adult healthcare, especially in rural and remote areas that lack specialist services, necessitating long travel distances for essential treatments. AYAs reported that accessing mental health services can be particularly challenging, worsened by a shortage of psychiatrists skilled in managing cases involving complex comorbidities. Participants noted that adult services frequently lack the capacity or expertise to address the multifaceted needs of these patients, leaving under-resourced GPs to fill the gap, often inadequately. As a result, many AYAs experienced discontinuity in care, insufficient support, and an increased risk of being lost to follow-up during transition.
Financial difficulties significantly impacted AYAs during healthcare transition. According to HCPs, AYAs struggle to afford adult care including expenses for hospital visits, medications, and specialist appointments. As they “aged out” of coverage under their parents’ insurance, AYAs reported additional expenses which they became responsible for. Medications that were previously low-cost or free in paediatric settings became expensive in adult services, adding to the financial strain. HCPs noted that publicly funded services, particularly psychiatry, were less accessible in adult care, leading some families to pursue costly private specialists to avoid long waiting lists and gaps in care. Travel expenses to appointments and potential income loss from taking time off work further added to AYAs’ financial challenges. AYAs reported needing to work multiple jobs and make compromises in their healthcare decisions to cope with these financial constraints. Balancing new responsibilities such as rent and bills in some instances exacerbated their reliance on parents and/or carers, impacting their independence.
Navigating the adult healthcare system posed significant challenges for AYAs and their families. Families reported struggles with unresponsive specialists, lack of communication between departments, and the need to frequently turn to private health care due to limited public options. This disjointed approach contributed to medical burnout and frustration, as parents and AYAs were required to take on the complex task of coordinating care without the comprehensive support they previously received.
Individuals’ understanding of both the transition process and medical conditions were identified by participants as factors that influenced the transition process. Adult HCPs highlighted that AYAs, paediatric HCPs, and often even adult HCPs may not always be aware of the specific need for different specialties of care. While some AYAs reported that they felt well-informed about their conditions and medical terminology, others lacked this knowledge, contributing to a reduced understanding of the importance of specialised care. Since adult HCPs generally have more experience with adults and an aging population, participants noted that they may lack knowledge about conditions with paediatric onset, especially for rare diagnoses. Some participants reported that HCPs may be unaware of the unique needs of AYAs who are still learning about their health and navigating the healthcare system. Participants reported adult HCPs as lacking empathy for the anxiety or fear AYAs experience when transitioning their health care treatment and management to the adult system.
Participants reported that healthcare transition is often marked by differing expectations and responsibilities between AYAs and HCPs. This project found that a disconnect regularly exists between adult HCPs’ expectations of an AYAs’ readiness for independence and the AYAs’ capacity and preparedness for managing their healthcare needs. AYAs noted that adult HCPs may assume AYAs are fully capable of self-management, expecting them to handle appointments, medication adherence, and health monitoring on their own. AYAs inability to handle the responsibilities had the potential to lead to misunderstandings and inadequate support, where missed appointments or non-compliance are misinterpreted as disengagement rather than a need for further guidance.
AYAs’ self-management skills and transition readiness were identified as factors that may influence successful healthcare transition. Many AYAs acknowledged the importance of increasing independence in managing their healthcare. However, there was a delicate balance regarding parental and/or carer involvement and concerns that their presence might undermine AYAs perceived independence. Some AYAs preferred and felt confident to manage their care independently, while others valued their parents’ continued involvement as a support system. HCPs also recognised the need to encourage self-management and independence, acknowledging that the appropriate level of parental and/or carer involvement is likely to be unique for each AYA and may require a flexible approach. AYAs referred to strategies that enabled them to become more independent in managing their care, such as keeping folders of important medical information to take to each appointment, taking notes during appointments, and using calendars or reminder systems for appointments.
Many AYAs reported experiencing significant life changes contemporaneous to healthcare transition, such as leaving home, attending university, or beginning a job. They reported that having to negotiate competing responsibilities posed challenges in managing frequent medical appointments, which could potentially lead to gaps in healthcare continuity. The need to negotiate and navigate these new responsibilities such as using sick leave or arranging time off work for appointments was described as further complicating their ability to maintain a consistent appointment schedule. Both HCPs and parents recognised the increased risk of AYAs falling through the cracks due to reduced parental oversight, the demands of new responsibilities, and the impact of mental health issues.
Proposed transition compass intervention
Our findings highlight that healthcare transition is multifaceted and presents a major challenge due to the involvement of two very different healthcare systems. Developing a straightforward solution across both paediatric and adult healthcare settings is unrealistic given the system complexity. Instead of attempting to completely overhaul one or both systems, the determinants of transition identified in this study suggested that an intervention focused on developing self-management skills for AYAs could be an effective and feasible approach (Fig. 1). This approach would empower AYAs to become more independent in managing their healthcare needs and increase their confidence in navigating the intricacies of the healthcare system. We aimed to develop an intervention that could be applied universally, ensuring that AYAs who are independent in managing their own care have access to support if needed, whilst being able to identify those at risk of disengaging from care and directing them to more intensive assistance as needed. We explored participants’ views on the proposed components of the Transition Compass intervention including automated messaging support, connection to a transition coordinator, and education modules.
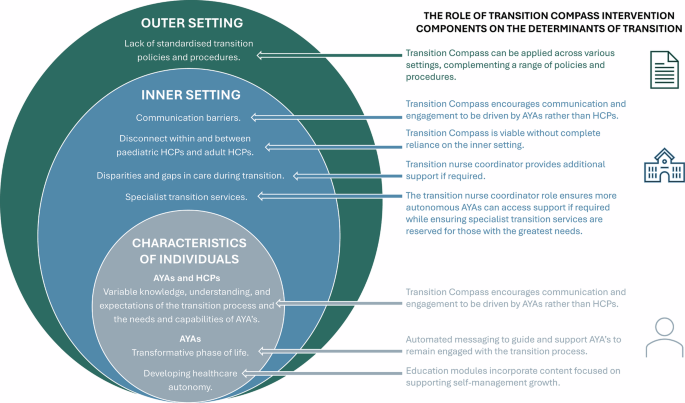
Key determinants influencing the healthcare transition process: Individual, inner setting, and outer setting CFIR domains and the corresponding role of Transition Compass intervention components.
Automated messaging intervention and associated transition coordinator
An automated messaging intervention and associated transition coordinator were generally viewed as an acceptable and appropriate approach to support AYAs during healthcare transition. However, participants identified several factors to consider in its design. Participants noted that individuals have varying preferences for communication methods. While some may appreciate phone calls, others may have an aversion to them. Offering various communication channels within the intervention and allowing participants to select their preferred methods, such as phone calls, emails, and text messages, may accommodate these diverse preferences and enhance the intervention’s appeal. Allowing participants to select how frequently they receive communication can tailor the intervention to match their individual needs and preferences, ultimately improving their engagement and satisfaction.
AYAs emphasised the importance of using a warm, inviting, and informal tone in messages. They suggested that communication should feel personable and relatable to avoid coming across as inauthentic or robotic. Including informal elements such as graphics interchange formats (GIFs) and emojis was seen as a potential way to enhance relatability and engagement.
The transition nurse coordinator was identified by participants as an important component to enhance engagement with the intervention and to provide added support for those that need it. AYAs expressed concerns about perceiving automated messages, such as texts, as spam, leading them to ignore or dismiss unfamiliar messages. They suggested initially sharing information through a credible source, like a website or email, to establish the legitimacy and trustworthiness of the phone number sending the messages. Another suggestion for improving trustworthiness involved integrating a human connection into the messaging system, such as meeting the transition nurse coordinator. This way, AYAs could conceptually link the messages to the coordinator, enhancing trust in the communication process – putting “a face to the name”. Overall, participants welcomed the concept of AYAs having access to a transition coordinator for additional support. They emphasised the importance of either meeting the coordinator during the recruitment process or at least having a written or video introduction to establish familiarity with the human connection behind the messaging system.
Participants highlighted important considerations for the adaptability, accessibility, and cost effectiveness of a messaging system including consideration for individuals who may lose their phone, thus requiring an alternative method for maintaining contact. Limiting responses to yes/no options was perceived by some AYAs as a possible barrier to engagement. It was suggested that using open-ended responses, where appropriate, could encourage more detailed and meaningful feedback.
Education modules
The inclusion of education modules within Transition Compass was largely perceived as beneficial, and participants provided input on various design considerations. AYAs emphasised the significance of tone in maintaining engagement and effectively conveying information in education modules. While humour was appreciated for its ability to captivate attention, AYAs also valued straightforward, informative approaches that prioritise clarity and purpose. The importance of having HCPs advocating for and encouraging AYAs’ engagement with the education modules was also highlighted. Participants suggested the inclusion of accessibility features like sign language interpretation and high-contrast visuals, as well as providing written text along with visual aids such as infographics. To enhance engagement and resonance, AYAs highlighted the importance of going beyond surface-level information by employing a storytelling approach rather than a mere “information dump”. They suggested finding a balance between generic and specific content to ensure broad appeal and relevance to most users.
AYAs raised varied perspectives on using social media such as TikTok or Instagram as a platform for information and education. There was recognition of its potential for relatability but also concerns about its susceptibility to misinformation. Concerns were raised about potential embarrassment if health-related content unexpectedly appeared within algorithms among friends. One advantage that AYAs saw in social media was the ability to easily consume short, concise content. AYAs noted that this bite-sized format would make it easier for them to quickly absorb information and stay engaged with the content.
The importance of drawing inspiration from existing models while ensuring that the Transition Compass intervention offers a unique point of difference was emphasised by participants. However, they advised against reinventing the wheel, advocating for the use of relevant and pre-existing resources where possible. This may include adapting existing ideas to suit the specific needs and objectives of Transition Compass.
AYAs advocated for an approach to the educational modules that was both authentic and relatable. Opinions varied regarding whether the information should be delivered by an AYA or a HCP, with some proposing that having both AYAs and HCPs represented may enhance the relatability and credibility of the content. Additionally, emphasis was placed on youth-led design, highlighting the importance of materials created with or by young people. Participants also advocated for accurate branding of the education resources to reassure authenticity and trustworthiness, avoiding the appearance of spam.
A range of relevant education topics were suggested by participants. These included but were not limited to independence and responsibility, expectation management, managing uncertainty, attachment/grief, advocating/knowing your rights, burnout, sexual health, driving and risk-taking behaviour, mental health, finance, discrimination, alcohol and drugs, lifestyle (sleep, exercise, nutrition), and Medicare and health insurance.