

Every child deserves to see a doctor when they’re sick – no exceptions.
No child with cancer should go without treatment because of where they were born. No toddler with asthma should be left gasping for breath because their family can’t afford medication. No child should be denied a vaccine from preventable illnesses and diseases. No pregnant woman should be told to wait five years to get prenatal care: not only is it fundamentally ridiculous and nonsensical, but such a policy also leads to higher rates of infant and maternal mortality.
These aren’t just talking points. They’re deeply personal to people all across this country.
My own family has been traumatized by infant mortality, cancer, diabetes, suicide, polio, sepsis, Alzheimer’s, and other medical heartbreaks. As a child, I remember a classmate passing away, and it was tragic that he did not get the medical care he needed due to either lack of income or immigration status. To me, it didn’t matter. Whatever the reason, it felt horribly wrong and unfair then and still does.
While working at University Hospital (then Thomason General Hospital), the public hospital in El Paso, Texas, I witnessed firsthand the anguish of families trying to access care they couldn’t afford. As a result, I firmly believe that nobody should ever be denied health care due to income, race, gender, disability, geography, place of birth, or immigration status.
In my job, I learned about the Hill-Burton Act, which first established obligations for hospitals receiving federal funds to provide charity care, regardless of ability to pay or immigration status. This wasn’t just federal law – it reflected basic medical and societal ethics.
To assist our hospital emergency department maintain its Level I trauma center status and financial viability to serve all of the people in El Paso and surrounding areas, I worked closely with hospital leadership and our affiliated physicians from Texas Tech University Health Sciences Center on a variety of public policy issues related to Medicaid, disproportionate share hospital (DSH) payments, medical residency programs related to emergency care, other graduate medical education (GME) funding, maternal and child health (MCH) services, emergency transportation, community health centers (CHCs), substance abuse, and mental health programs.
Through the advocacy of University Hospital and other public hospitals across the country, Sen. Lloyd Bentsen (D-TX) worked with Sen. John Chafee (R-RI) and Rep. Henry Waxman (D-CA) on what is known as emergency Medicaid – a small but vital tool to reimburse hospitals when they provide emergency services, including labor and delivery care, to people ineligible for full Medicaid coverage due to their immigration status.
This provision, passed and signed into law in 1986 by President Ronald Reagan, acknowledges that hospitals should not be penalized financially for doing what human decency demands. As a result of the provision, hospitals can be reimbursed for life-saving treatments, such as those provided in emergency rooms or during childbirth, regardless of a patient’s immigration status. This funding helps offset unreimbursed uncompensated care costs for hospitals, and now accounts for just 0.4% of Medicaid spending.

That same year, Congress enacted the Emergency Medical Treatment and Labor Act (EMTALA), which requires hospitals to provide emergency care to all patients, regardless of ability to pay or immigration status.
For purposes of the current debate over the government shutdown, it is essential to make the point that emergency Medicaid does NOT provide health insurance coverage to undocumented immigrants; it simply offers reimbursement to hospitals that provide related emergency life-saving care to immigrants in the emergency department.
These emergency care provisions have been federal law for nearly 40 years.
In 1996, the Personal Responsibility and Work Opportunity Reconciliation Act (PRWORA) was passed, which bans undocumented immigrants from receiving public benefits. It also imposed a five-year waiting period before lawfully present immigrants – including children and pregnant women – could qualify for Medicaid. Quite frankly, that law has been a step backwards, but it is the law. Immigrants do not receive health insurance coverage from Medicare, Medicaid, or the Children’s Health Insurance Program (CHIP).
Sen. Bob Graham (D-FL) introduced legislation to allow states the option to waive the five-year waiting period and cover legal immigrant children and pregnant women. Sen. Graham felt that no child with cancer, asthma, or in need of a vaccine should be asked to wait five years to receive care, as that could be a life sentence. He also felt that the policy, which blocked a pregnant woman from receiving prenatal care for five years, was ludicrous and nonsensical, but also dangerous.
The following year, CHIP was established and has proven to be one of the most successful child health initiatives in American history. In 1997, more than 15% of children in the U.S. were uninsured. Following the passage of CHIP and in partnership with Medicaid, the uninsured rate for children declined by more than two-thirds, dropping the rate below 5% by 2016. That’s not just a statistic – it is a life-changing improvement in the lives of children.
More than a decade later, the CHIP Reauthorization Act (CHIPRA) of 2009 was passed and signed into law by President Barack Obama and included provisions by Sen. Jeff Bingaman (D-NM) that allow states to cover pregnant women through CHIP and to use Express Lane Enrollment to streamline enrollment and retention for eligible children.
Furthermore, Sen. Graham’s bill to give states an option to waive the five-year waiting period for legal immigrant children and pregnant women was also included in CHIPRA.
These steps toward reducing the uninsured rate are essential because the research is clear: providing health insurance coverage to people saves lives. Anything less and steps in reverse are not just cruel, they are economically irrational, medically irresponsible, and morally indefensible. It is a betrayal of our most basic values.
At this moment in time, we stand at a critical crossroads. Without action to protect health coverage, our nation will head dramatically backwards in terms of denying health care coverage and access to care to millions of people. Despite the rhetoric of the Trump Administration and some in Congress, the health care fight in the government shutdown is NOT about extended health care to undocumented immigrants.
What it is actually about is whether we will protect over 14 million people from losing the health coverage they already have through federal Medicaid and CHIP cuts, expiration of Affordable Care Act (ACA) Marketplace subsidies, and other cuts to vital health care programs and services.
The stakes could not be higher.
To explain, the “One Big Beautiful Bill” (OBBB), passed earlier this year and signed into law by President Trump on July 4, 2025, includes nearly $1 trillion in cuts to Medicaid and CHIP. If left in place, those cuts would result in an estimated 10 million people losing coverage, primarily low-income children, families, people with disabilities, and seniors in long-term care.
At the same time, key provisions of the Affordable Care Act (ACA) that make private coverage affordable for working families are also set to expire. Without Congressional action, another 4 million people could lose coverage when ACA subsidies lapse.
Congressional Democrats have demanded that this coverage be restored and protected in the end-of-year budget negotiations. Again, the more than 14 million people at risk by OBBB’s Medicaid and CHIP cuts and the failure to extend ACA subsidies are NOT undocumented immigrants. The restrictions on access to public health programs for undocumented immigrants were established in the PRWORA back in 1996 and remain in place today.
Despite assertions by Vice President JD Vance, the official X account of Senate Republicans, and House Speaker Mike Johnson (R-LA), nothing being proposed by congressional Democrats, including reversing the cuts in H.R. 1, would alter that legal framework.
According to Sen. Patty Murray (D-WA):
Undocumented immigrants are not eligible to enroll in federally funded health coverage under existing law or Democrats’ funding proposal – but millions of American citizens will see their health care premiums double next year if Republicans keep refusing to act.
So why the misdirection and finger-pointing at health care for immigrants?
For one, it polls well with the base, even if it has been the law since 1996.
Rather than defend the indefensible truth – stripping coverage from over 14 million people, including children – former Speaker Newt Gingrich recognizes that distraction and division are better political strategies.
Sen. Mark Kelly (D-AZ) exposes the strategy for what it is.

The reality is that Democrats are arguing for a reversal of the Medicaid and CHIP cuts in H.R. 1 (OBBB) and for extending ACA subsidies to protect the health coverage of 14 million people.
Beyond the Administration’s false claims, some groups like the Paragon Institute have pushed misleading talking points suggesting that reversing Medicaid and CHIP cuts or extending ACA subsidies would somehow increase federal health care spending on “unlawful immigrants.” However, these claims also collapse under scrutiny. They rely on mischaracterizations of how public programs work, what federal law allows, and who receives coverage.
As an example, Paragon Institute misrepresents emergency Medicaid as a form of insurance for undocumented immigrants. As noted above, it’s not. Again, it’s a narrow reimbursement mechanism that allows hospitals to recoup costs when providing emergency care – such as a heart attack, traumatic injury, or labor and delivery – to people ineligible for full Medicaid benefits. It exists because hospitals, as required under EMTALA, provide care to anyone who presents in need, regardless of their status or ability to pay. Reimbursing hospitals for following the law is not a loophole: it’s a necessity. However, let’s be clear: it does not provide ongoing health coverage to patients and has never done so.
Paragon and others also like to point to the reality that a few select states are using federal funds to cover undocumented immigrants. Although I applaud those states for striving to ensure all people in their state have access to care and are not needlessly dying due to a lack of coverage, opponents are purposely misleading and disingenuous in arguing that congressional Democrats are trying to open up federal dollars for such coverage.

What’s being cast as a debate over “illegal immigration” is, in reality, a high-stakes decision about whether millions of Americans will get to keep seeing their doctors, filling their prescriptions, and taking their children in for checkups. The political theater hides the policy cruelty.
Stripping away health coverage from children, pregnant women, people with disabilities, and working families doesn’t strengthen the country. It weakens it. It’s a blueprint for more suffering, more preventable deaths, and higher long-term costs for all of us.
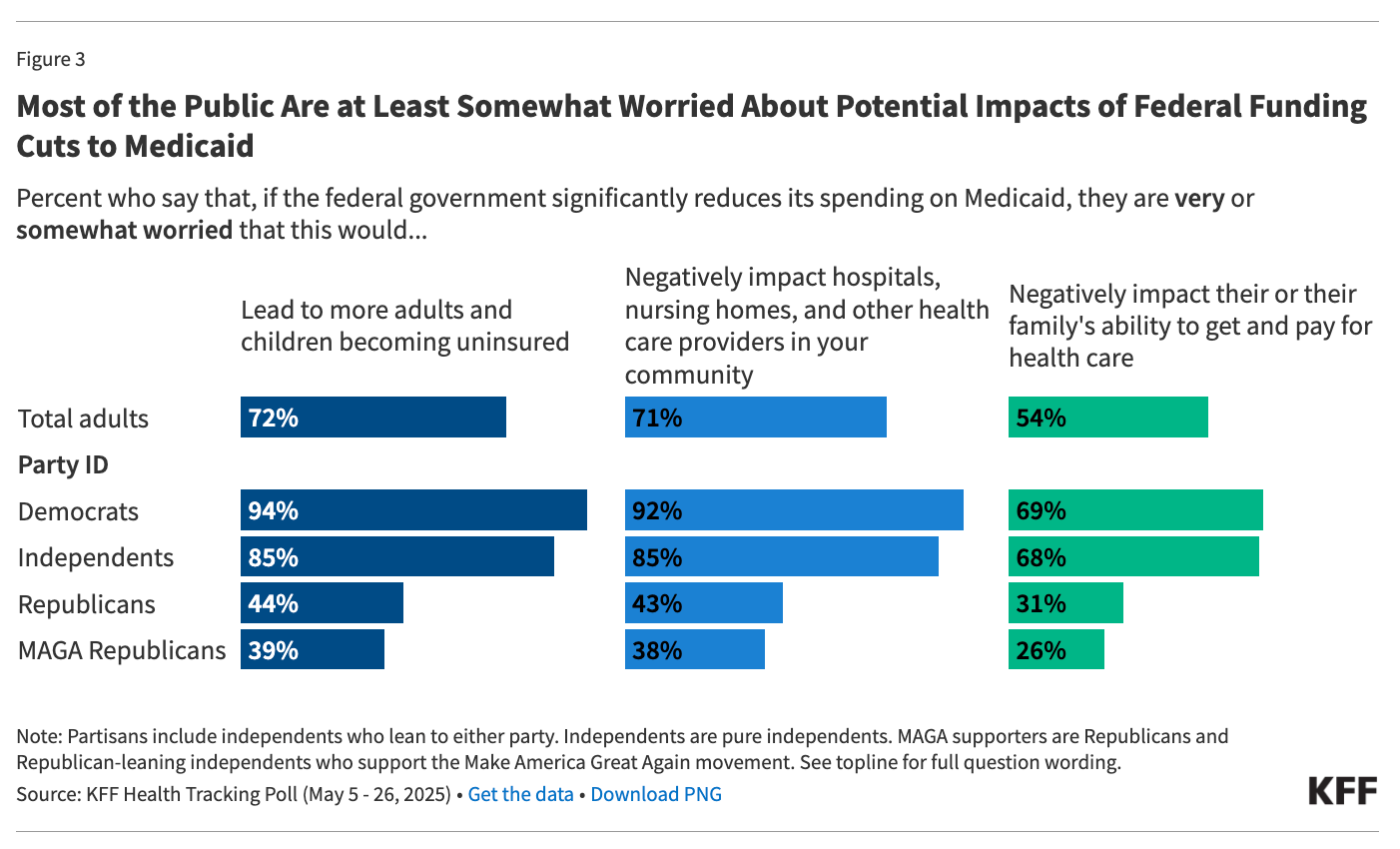
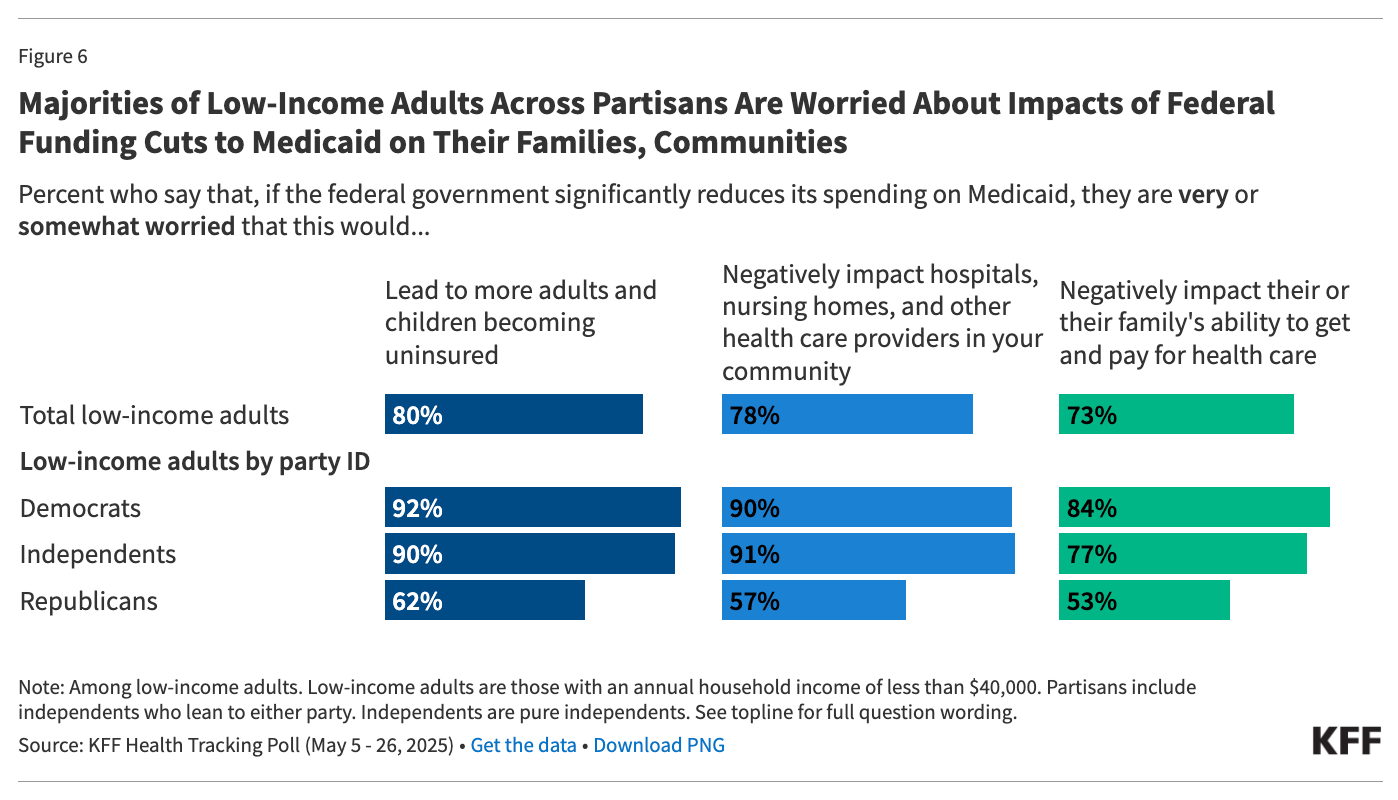
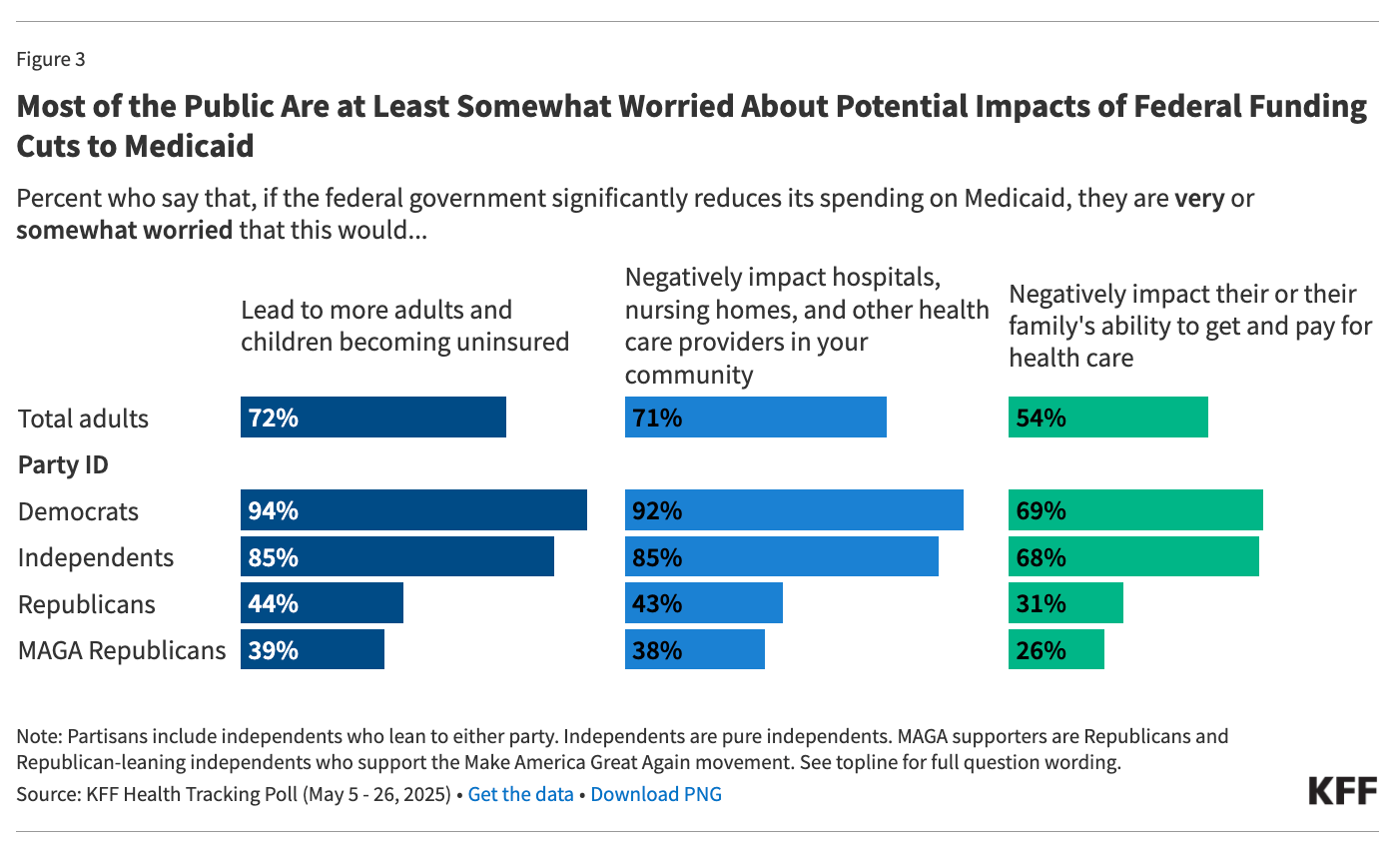
For these reasons, it is clear that the American people oppose the nearly $1 trillion in Medicaid and CHIP cuts and support extending the ACA Marketplace subsidies that would otherwise expire. The following charts highlight the KFF polling on these issues.
In moments of crisis like this government shutdown, we sometimes discover who we are as a country and who we are willing to protect or leave behind.
We can choose fear, scapegoating, and disinformation. We can distract the public with tired myths about immigrants receiving benefits they are legally excluded from. We can pretend that taking health care away from over 14 million people, including millions of children, is somehow an act of fiscal responsibility. We can tell hospitals not to provide life-saving care to the uninsured, including undocumented immigrants, and allow them to die.
Or, we can choose the values we say we believe in: dignity, fairness, compassion, and life itself.
The real question before Congress isn’t whether to expand health care to undocumented immigrants. That’s not on the table in this shutdown.
The question is whether we will allow cruelty and confusion to drive policy decisions that will devastate families, reverse decades of progress, and disproportionately harm children: all for the sake of a talking point.
We have seen this rodeo before.

According to CBO, under the reconciliation law (H.R. 1), at least 10 million people would lose health coverage compared to the baseline, and if ACA Marketplace subsidies are allowed to expire, that number would rise to more than 14 million. This isn’t theoretical. It’s a policy choice with devastating, measurable consequences.
We’ve been here before, and we know how to move forward. Medicaid and CHIP have shown us what’s possible. The ACA has proven that coverage can be expanded and made more affordable for millions. We should build on and protect that progress – not reverse course and destroy it.
And while we’re discussing the protection of health coverage for millions of U.S. citizens, we urge making CHIP permanent, as it would protect coverage for the millions of children who depend on it, year after year, without the threat of political gamesmanship when it is set to expire in 2029. Why wait and allow CHIP to expire for months due to political inertia, as occurred in 2007 and again in 2017?
In this year’s budget negotiations, we should have an honest discussion and debate about the future of health care in this country. There are real, honest, and worthy debates that should be had about how health care is delivered and financed in this country, but wasting time and energy on red herrings, lies, and misdirection fails us all. The stakes are far too high. It is past time to have the necessary adult conversations that include the future of children’s health.