This is the online version of STAT’s weekly email newsletter Health Care Inc. Sign up here.
Hello! The newsletter didn’t come out yesterday in honor of MLK Day, but we’re back right after Indiana University became national champions. I also want to know why the maple leaf emoji is used so frequently in patients’ medical charts. Palm over face emoji. Runner emoji, mail emoji: [email protected].
*siren emoji* NEW TRUMP HEALTH PLAN *siren emoji*
Don’t spend a lot of time analyzing President Trump’s “Great Healthcare Plan.”
After Trump released the 825-word “fact sheet” last week, PR reps and others filled my inbox, ready to offer just about anyone to give a take on it. But it’s less of a plan, and more of a political document, just like the budgets that every president releases.
This plan, in particular, is a piece of paper that can be waved around during a midterm election year in which Americans are getting hammered on their health care premiums. It’s the Trump administration learning what medical loss ratios are, and wanting hospitals to print out pricing spreadsheets and plaster them on their walls.
But it would not reshape the structure of Medicare, Medicaid, or the health insurance plans people get through their jobs. It would not repeal Obamacare. And it would require Republicans in Congress to act, even though they have explicitly shot down some of these ideas in the recent past — like the most-favored nation policy for drug prices.
Many people will live their lives, never having read a word of it. And that’s OK. You don’t have to either. But my colleagues Daniel Payne, John Wilkerson, and I did just in case.
Hospitals kept a low profile, on stage and off
Usually at the J.P. Morgan Healthcare Conference, nonprofit hospital presentations are full of chest-thumping about market share and investment income war chests. This year, not so much, my colleague Tara Bannow reports from the confab.
Tara searched her Otter transcripts and found 17 examples of executives talking about stability or consistency. Ascension pointed to its “stable operating performance,” and SSM Health touted its “culture of stability.” And instead of bragging about being more profitable than its peers, AdventHealth declared that “it all begins and ends with consistent financial performance.”
Tara found a similar vibe at a swanky yacht club on the sidelines of JPM, when hospital leaders enjoyed wine and caviar and then listened to CMS Administrator Mehmet Oz and four of his top officials speak. Even though Oz dismissed concerns about a $1 trillion cut in Medicaid funding over a decade as “catastrophizing,” insinuated that a lot of Medicaid enrollees are couch potatoes, and called state directed payments “legalized money laundering,” most executives nodded along and, talking to Tara afterward, declined to push back on any of it.
Hospitals were somewhat coy over their use of AI. AdventHealth is transforming its 13,000 inpatient rooms into “virtual care smart rooms.” Intermountain has processed over 70,000 IT help desk tickets using an AI tool.
But hospitals’ presentations also showed the technology’s potential to exacerbate the divide between the haves and the have-nots. Wealthier systems like Mayo Clinic and Cleveland Clinic had plenty to say about how they’re deploying AI, whereas those just trying to break even, like Ascension, CommonSpirit, and SSM, didn’t mention it as much.
It’s a theme Eric Klein, a lawyer who co-leads Sheppard Mullin’s national health care practice, hears frequently: Hospitals that can’t afford to invest in AI “need to cut services or partner or figure out a way to raise enough capital to do the transformative work with AI.”
Klomp and circumstance
While in San Francisco, Tara spoke with Chris Klomp, the director of Medicare at CMS, who reports to Oz.
One of the Trump administration’s first actions on Medicare Advantage was expediting audits known as risk adjustment data validation, or RADV. But officials announced this program even though CMS has been stuck in litigation over those same RADV audits. So Tara asked him, what’s up with all that?
Klomp: “We can continue the audits under the status quo. For us to audit all the claims would probably be physically impossible because it would cripple the system. Like, literally, there would be no one providing care because everyone would be doing audits. And so we’re working on some alternatives. I won’t talk about those especially because they’re still in play.”
“I’d say the bigger principle is we want patients, lawmakers, the American people to have confidence that MA is being a wise steward of the taxpayer resources that we administer, that that industry makes use of to provide care. It’s pretty clear that right now, trust, for whatever reason, has been compromised. We are serious about ensuring a restoration of integrity in that program. And there are a variety of ways to do that. RADV is one tool of many. But we’re totally serious about it, and we’ve hardly relented.”
Going up while going down
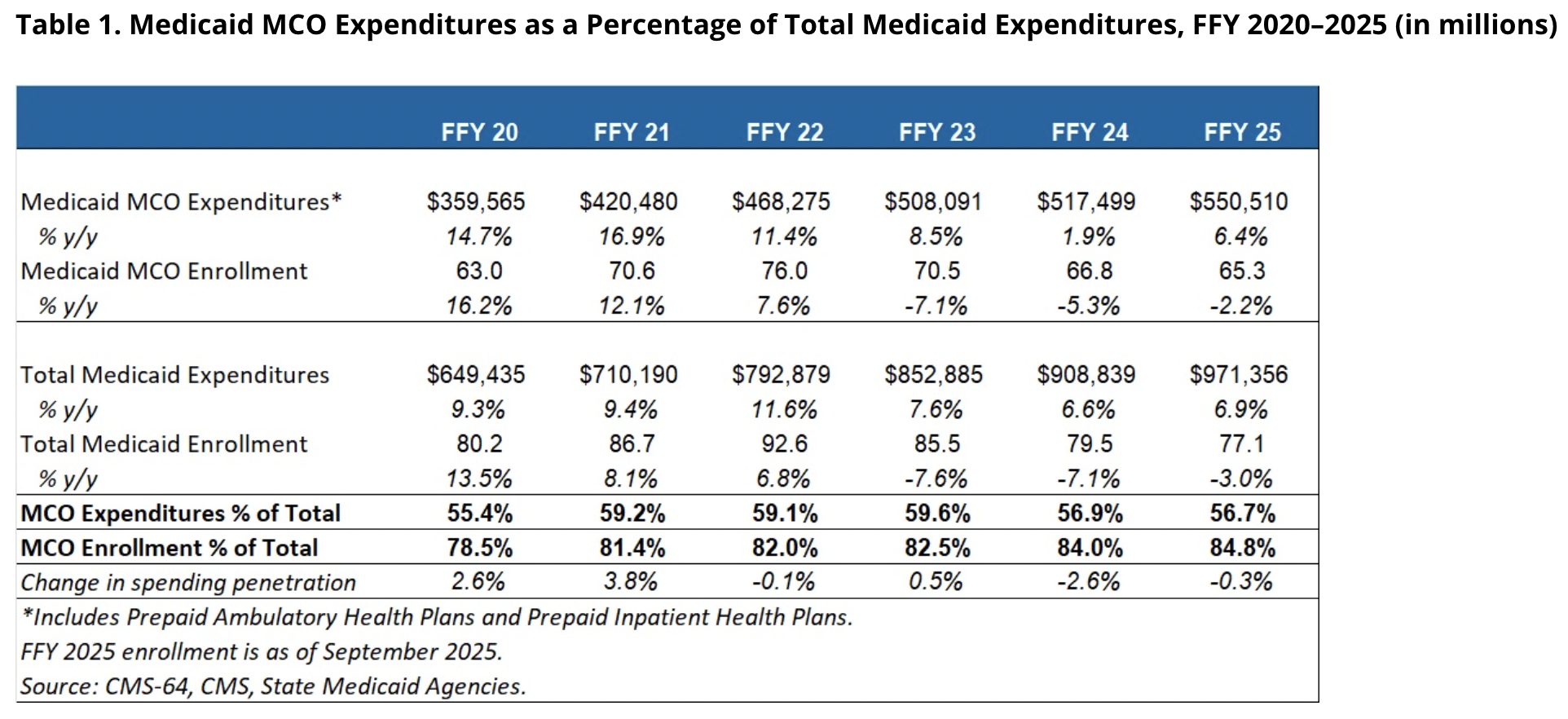
Total Medicaid spending increased by 7%, hitting almost $1 trillion in the 2025 federal fiscal year, according to federal data analyzed by the consulting firm Health Management Associates. That happened even though Medicaid enrollment dropped by 3%. What gives?
The explosion of state directed payments.
It’s not the prices? It kinda still is?
Last summer, CMS’ actuaries informed us we are now a $5.3 trillion health care system. Those numbers remained the same in their final 2024 analysis released last week.
Mike Chernew, a health policy professor at Harvard Medical School, wrote an accompanying article in Health Affairs explaining how the growth in health spending in 2024 was “not the prices, stupid” — a riff on the famous 2003 article that details how the U.S. spends more on health care than other countries simply because it charges higher prices.
There’s a lot of truth to Chernew’s thesis: CMS actuaries told reporters last week that “non-price” factors like use and intensity of care were bigger factors in the spending growth. Chernew also writes about hospitals buying physician practices and the AI coding wars driving up spending.
But there’s some contradiction in Chernew’s article. He writes the “use of expensive products” is a “nontrivial” factor of higher spending. “Expensive” implies the products have high prices to begin with. The fact that we spent almost $15,500 per person on health care in 2024, compared with $4,600 in 2000, indicates the U.S. still pays way more for basic health services and drugs than other countries — we are just also using more of them lately.
In addition, prices for hospital care — where a good chunk of our health care spending goes — increased by 3.4% in 2024. That was “the highest rate of increase since 2007,” actuaries wrote. Hospital executives blatantly said in 2023 that they planned on hiking prices by a lot in the wake of the pandemic. With many of the newer negotiated contracts coming into effect in 2026, it’s not unreasonable to think prices are going to jump by a considerable amount in future reports.
Industry odds and ends
- Kaiser Permanente agreed to pay $556 million to settle allegations that it pressured its doctors to add diagnoses to the medical charts of Medicare Advantage patients. It’s the largest-ever Medicare Advantage fraud settlement secured by the Department of Justice. Read more from Tara.
- Hospitals are pressuring CMS to change a document that says all applicable hospitals “are to respond” to a survey asking them about their drug costs. In November, CMS moved forward with the outpatient drug cost survey, against hospitals’ wishes — even though the Supreme Court suggested CMS conduct it and even though it is technically required by federal law.
- A small study of electronic health record data among University of California San Francisco physicians finds that AI scribes boost revenue by roughly $3,000 per physician annually — less charting allows physicians to see more patients.
- Pharmaceutical giant Genentech dumped the pharmacy benefit manager for its employees — one of the big three — and replaced it with smaller PBM Rightway, Max Bayer of Endpoints reports.
- Nearly 15,000 nurses who work at New York City’s major hospitals went on strike last week. Nurses unions have said this is the largest nursing strike ever in New York City. Starting today, another 31,000 Kaiser workers also are set to strike at facilities across California and Hawaii.
- “Level-funded” plans have become more popular with employers, but these health insurance arrangements often come with “silent risks,” insurance expert Frank Pennachio writes in BenefitsPRO.
- Boston Scientific is acquiring Penumbra for $14.5 billion. Penumbra makes cardiovascular medical devices, so this deal will give Boston Scientific — already one of the biggest heart and vascular device makers — an even stronger hold in the cardiovascular market.
The Meme Ward