

A total of 3479 unique articles were retrieved from the database search. Forty-eight articles were assessed against the full-text eligibility. Twenty-eight articles were included in the review after excluding articles based on the inclusion and exclusion criteria. The PRISMA diagram presents the number of studies retrieved (Fig. 1).
Study characteristics of the included articles are summarised in Table 2. While most were conducted in the USA (n = 6) [33,34,35,36,37,38], followed by Canada (n = 4) [39,40,41,42], Australia (n = 2) [24, 43], Turkey (n = 2) [44, 45], and China (n = 2) [46, 47]. The remaining studies were conducted across several other countries. The majority of the studies (n = 18) [33, 35,36,37, 41, 42, 44,45,46,47,48,49,50,51,52,53,54] used a quantitative design, using surveys or questionnaires, with a few mixed methods studies (n = 3) [43, 55, 56], qualitative studies (n = 5) [24, 39, 40, 57, 58] and descriptive studies (n = 2) [38, 59]. Most studies included participants with a nursing background (n = 24), while the remaining studies included occupational therapists [57], optometrists [48], speech pathologists [24], and the collective term allied health professionals [54]. Most studies utilised specific frameworks to support the integration of genetic strategies, including: Canadian Nursing and Genomics Framework (n = 3) [39, 40, 42]; Rogers’ Diffusion of Innovation Theory (n = 2) [46, 47]; while Lewin’s Action Research Principles [43]. The Consolidated Framework for Implementation Research [44], Theoretical Domains Framework (TDF) [24], R.I.S.E. 2 Genomics Framework [58] and Johnson and Aragon’s (2003) Framework [39] were each referenced in one study.
Empirical strategies
Various strategies have been employed and tested to support the integration of genetics among allied health professionals, and each strategy is described in relation to the genetic context (Table 3). The empirical strategies include workshops (n = 1) [43], web-based education and reminder systems (n = 1) [44], leadership development (n = 1) [58], and the involvement of senior staff to support genetic integration. The integration of educational and online resources was a common strategy to support genetic literacy, including web-based tools and learning platforms (n = 7) [33,34,35,36, 43, 44, 52, 55]. Curriculum development and review (n = 3) [34,35,36], undergraduate education programs (n = 2) [35, 36], and postgraduate education (n = 4) [33, 34, 55, 58] were associated with significant improvements in participants’ genetic knowledge. Finally, case-based learning approaches supported genomic literacy, evaluating both genetic knowledge and its application in practice (n = 3) [34, 36, 52].
Conceptual strategies
Several conceptual strategies were suggested to enhance genomic literacy among healthcare professionals, including: education and training programs (n = 9) [24, 36, 46, 47, 50, 51, 57, 59, 60], educational resources (n = 9) [24, 37, 38, 45, 47, 49, 54, 57, 60], interdisciplinary collaboration (n = 9) [24, 38,39,40, 42, 48, 50, 57, 60], curriculum development (n = 7) [37, 39, 40, 42, 53, 56, 60], continuing education (n = 6) [38, 48, 50, 51, 56, 59] (Table 4). The influence of nurse educators, senior staff, and expert support systems (n = 7) was identified as a strategy to support integration of genetics [24, 41, 45, 46, 50, 56, 60]. There were also other strategies proposed such as development of standalone or integrated courses (n = 6) [41, 48, 49, 51, 53, 59], international collaboration (n = 5) [47, 49, 51, 56, 59], tailored education approaches (n = 4)[24, 37, 45, 46], professional development opportunities (n = 4) [24, 42, 49, 57], development of genomic literacy toolkits and evaluation tools (n = 4) [40, 49, 53, 56], undergraduate education (n = 4) [38, 47, 53, 54], postgraduate education (n = 3) [39, 45, 49], clinical supervision and experiential learning (n = 2) [24, 60], use of case studies as practical learning tools (n = 2) [51, 59], raising awareness and fostering positive attitudes (n = 2) [40, 47], co-designed educational content (n = 1) [48], lectures delivered by genetic counsellors (n = 1) [54], examination of accreditation standards (n = 1) [41]. Digital platforms (n = 1) are suggested to support educational delivery [38], and advocacy efforts (n = 5), including securing financial investment [40], policy development [50, 56], and alignment with national and international genomic strategies [40, 53, 56] were also identified to support the integration of genetics.
Theoretical Domains Framework
The empirical and conceptual strategies were mapped to the domains of the TDF, categorising factors that influence the integration of genetics into practice. Both empirical and conceptual strategies reported the use of several resources. For example, within the Environmental Context and Resources domain, educational resources were a common strategy used among the empirical strategies [33, 34, 43, 55]. These included online modules, toolkits, and self-directed learning platforms designed to improve accessibility and engagement among health care professionals. Social Influences and Social/Professional Role and Identity were also frequently targeted domains among the strategies identified in this review. Some studies reported the involvement of senior staff and leadership [43, 50], while others proposed the use of genomic champions and interprofessional training to promote peer influence and support [24, 42]. These strategies recognise the importance of fostering a supportive environment for healthcare professionals.
Across the included empirical strategies, the most frequently mapped TDF domain was Knowledge (n = 10), highlighting its importance in implementation strategies. Environmental Context and Resources (n = 4) and Social/Professional Role and Identity (n = 4) showed moderate representation. Memory, Attention and Decision Processes (n = 3), Skills (n = 3), Social Influences (n = 2), Behavioural Regulation (n = 2), and Beliefs about Capabilities (n = 2) were mapped less often (Table 3). While among the identified conceptual strategies, Knowledge (n = 12) was again the most frequently, followed by Social/Professional Role and Identity (n = 9), Environmental Context and Resources (n = 7), Skills (n = 6), Social Influences (n = 5) and Beliefs about Capabilities (n = 4) were moderately mapped to the conceptual strategies. Belief about Consequences (n = 1), Behavioural Regulation (n = 1), and Memory, Attention and Decision Processes (n = 1) were mapped less often.
Overall, TDF domains such as Knowledge, Social Influences, and Social/Professional Role and Identity were the most frequently represented. These domains were associated with various strategies, for example, Social Influences was mapped onto support system, collaboration, leadership and supervision, including the involvement of genomic champions to promote engagement with genetic and genomic practices (Fig. 2). Intentions, Reinforcement, Optimism, Emotion and Goals domains were notably absent. Meanwhile, domains such as Skills, Beliefs about Capabilities, Beliefs about Consequences, Memory, Attention and Decision Processes, Environmental Context and Resources and Behavioural Regulation were fairly represented across the identified strategies.
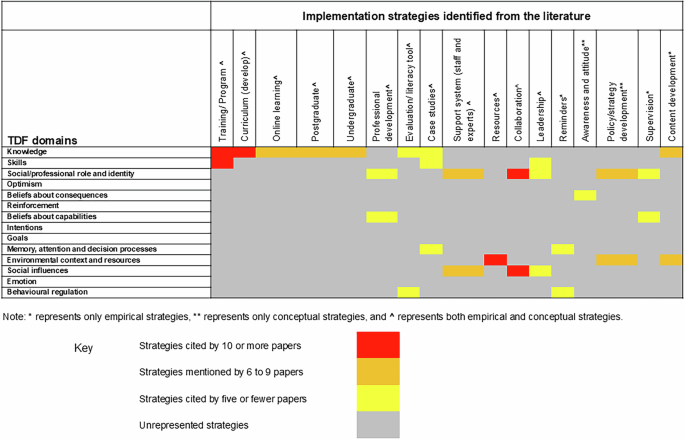
Heat map on implementation strategies and associated TDF domains.