
The Institutional Review Board (IRB) of the Università della Svizzera italiana in Lugano has reviewed and approved the research protocol (CE 2023 28). All research activities were conducted in accordance with the ethical guidelines and regulations set forth by the IRB. Participants were provided with an informed consent document, and their voluntary participation was obtained before any data collection activities commenced. All participants were over 18 years of age.
Data sampling
The data are drawn from responses to a survey of residents in Switzerland representative of the population aged 18 or above. The questionnaire was developed by the Institute of Communication and Health (ICH) of the Università della Svizzera italiana in Lugano, in collaboration with the Swiss Federal Office of Public Health. In the last phase of finalizing the questionnaire, ten test interviews were conducted. Data were collected by Polyquest AG, Berne. The contractor selected from an existing representative online panel persons for the survey. Due to a clear underrepresentation of persons with a low level of education, the original sample was completed by an additional 100 persons from the lower education strata, resulting in a final sample size of N = 1,713. Response rate was 35%. Interviews were conducted online. There was an intentional overrepresentation of participants from the French- and Italian-speaking regions of Switzerland to provide a better data basis for separate and comparative analyses of the linguistic regions. Field time was March 8–18, 2018, which preceded the Covid-19 pandemic so the prominence of vaccination and the misinformation associated with that period were not present. It is certainly possible that the number of people displaying high levels of misinformation could have changed, but we believe that the associations examined here will still obtain.
MeasuresObjective vaccination knowledge
As an objective, performance-based measure linked with health literacy, the vaccination knowledge test developed by Zingg und Siegrist was used19. The recommended version was used with nine knowledge items in the form of assertions that respondents were asked to say were true, false, or “I don’t know”: Vaccines are superfluous, as diseases can be treated (F); Without broadly applied vaccine programs, smallpox would still exist (T); The efficacy of vaccines has been proven (T); Children would be more resistant if they were not always vaccinated against all diseases (F); Diseases like autism, multiple sclerosis, and diabetes might be triggered through vaccinations (F); The immune system of children is not overloaded through many vaccinations (T); Many vaccinations are administered too early, so that the body’s own immune system has no possibility to develop (F); The doses of the chemicals used in vaccines are not dangerous for humans (T); Vaccinations increase the occurrence of allergies (F). The analyses use categorized groups based on the number of correct, incorrect, and “don’t know” answers. On average, respondents gave 4.92 (SD = 2.71) correct answers, 2.41 (SD = 2.24) incorrect answers, and 1.67 (SD = 2.06) don’t know answers.
A second objective knowledge variable was constructed to distinguish those who are misinformed (gave a wrong answer (answering “false” to a true item or “true” to a false one) from those who were uncertain about knowledge items (answering “I don’t know”). The number of wrong answers was subtracted from the number of “I don’t know” answers to give a measure labelled “Net Uncertainty”. The measure ranged from − 9 (highly misinformed) to + 9 (highly uncertain) with a mean of 0.73 (SD = 3.34).
Self-perceived or subjective health literacy
Subjective health literacy, or the self-perception of one’s ability to find and process vaccination information was measured by three items from the HLS-EU 47 that referred explicitly to vaccination and is interpreted as an indicator of a vaccination-specific measure of health literacy. The items asked about how simple it was to know why one needed vaccination, which vaccinations one needed, and to decide whether to get the flu shot annually as recommended. Scales ran from 1 to 4, with 1 indicating it was very easy, 2 fairly easy, 3 fairly difficult and 4 very difficult, with no option to give a neutral answer. For a composite measure the three scales were reversed (so as to have high values represent high subjective health literacy) and averaged (alpha = 0.69; M = 3.1, SD = 0.67).
Beliefs
Two belief measures were constructed from a 20-item battery of vaccination beliefs to which a participant could agree or disagree on a 5-digit scale. A factor analysis identified three factors, from which two index measures were developed. The first factor, on which 9 items load, describes the historical and universal importance of vaccination—It is irresponsible to others not to be vaccinated; Without vaccination our lives would be shorter; Eradication of infectious diseases is a desirable goal; Carefree world travel is possible because of vaccinations; The discovery of vaccination against infectious disease is a major medical achievement; Eradication of smallpox and polio is a great benefit of vaccinations; Before vaccinations, high infant mortality brought untold suffering to people; There is no need to debate vaccination: its value is clear; It is best to follow the doctor’s advice on vaccinations. Agreement with the items reflects greater perceived benefits of vaccination. The second factor relates to individual biomedical aspects of vaccination, especially the risks associated with it. Five items load on this factor—Vaccination is dangerous because one is given a mild form of the disease; Patients are more likely to be injured by vaccination than other procedures; People are not told how dangerous vaccination is; Because vaccinations are derived from natural pathogens, something can easily go wrong; I trust normal medicines more than vaccines. Here, agreement reflects greater perceived risk associated with vaccination. The items loading on each factor were averaged to form measures of perceived benefits (α = 0.86, M = 2.10, SD = 0.69) and perceived risk (α = 0.84, M = 3.44, SD = 0.82) of vaccination.
Attitudes
The attitude measure was a single item on the balance between advantages and disadvantages, measured with a 9-step scale defined by the endpoints that advantages or disadvantages dominate. High values indicate a dominance of advantages (M = 6.6, SD = 2.12).
Behavior
Two behavioral measures were constructed as outcome variables. The first measure was the Number of vaccinations a respondent self-reported to have had at the time of the survey, among a total of six basic or recommended vaccinations (tetanus, hepatitis B, measles, pertussis, meningitis, and influenza). The mean number of vaccinations received was 2.76 (SD = 1.82).
A second behavioral measure was Willingness to recommend vaccination, which was measured by asking participants whether they would recommend child vaccination for tetanus, pertussis, measles, hepatitis B, and meningitis. For each disease, a response using a 9-point scale (certainly would not recommend to certainly would recommend) was collected and the responses were averaged. Unidimensionality was assured via principal components (α = 0.90, M = 5.49, SD = 1.67).
Four background demographic variables were included in the study to control for age, educational attainment, gender, and prior professional medical experience (yes/no). The basic characteristics of the data set are shown in Table 1.
Data analysis
To test H0, a set of regression models was constructed to assess the effects of objective and subjective knowledge on perceived benefits, perceived risks, attitude toward vaccination, and the two behavioral measures. The models included objective knowledge, subjective literacy, and their interaction along with the four demographic control variables.
To examine Hypotheses 1 and 2, the focus of the present analysis, net uncertainty was added to objective knowledge and subjective literacy as a predictor. The effects of objective knowledge, subjective literacy, and net uncertainty were examined using linear regressions. The three predictors were mean-centered. All two-way interactions and the three way interaction were included in the analyses. Four demographic control variables—age, education, gender, and prior professional medical experience—were included.
Results
According to H0, subjective literacy should amplify the positive effects of objective knowledge. The regression results are summarized in Table 2.
A significant interaction effect is found for perceived benefits, perceived risk (marginal), number of vaccinations received, and willingness to recommend vaccination. For attitude, objective knowledge is associated with more positive attitude but the interaction with subjective literacy is not significant. Thus, for beliefs and behaviors, Hypothesis 0 is supported, consistent with prior research18.
The results of the regression models examining Hypotheses 1 and 2 are summarized in Table 3.
Beliefs: perceived benefits and risk
In the analysis of perceived benefits, objective knowledge, subjective literacy, and net uncertainty all have strong direct effects. These effects are moderated by interactions including the 3-way interaction of the knowledge variables. In order to characterize this interaction pattern, responses with the knowledge variables either 1 standard deviation below (low) or above (high) 0 were are shown in Fig. 1. For those with higher objective knowledge, net uncertainty has limited effect. Regardless of net uncertainty, these respondents report greater benefits of vaccination. Higher subjective literacy further increases perceived benefits. For those with lower objective knowledge, those who are more uncertain report less perceived benefits of vaccination but, as for those with greater objective knowledge, higher subjective literacy is associated with greater perceived benefits. Those with lower objective knowledge who are also more misinformed reflect a different pattern of responses. They report still less benefits of vaccination than other respondents, and increasing subjective literacy doesn’t affect these perceptions. The results are consistent with Hypothesis 1 and 2a. As proposed in Hypothesis 2b, subjective knowledge is not associated with higher perceived benefits for the low knowledge, misinformed respondents, differing from the respondents.
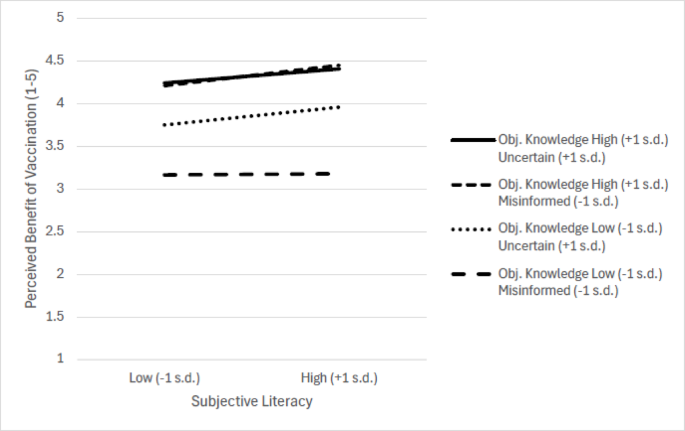
Objective knowledge/uncertainty and subjective literacy effects on perceived benefits of vaccination.
In the analysis of perceived risk, main effects of objective knowledge, net uncertainty, and subjective literacy are again significant, as is the interaction of objective knowledge and net uncertainly. Greater objective knowledge, greater subjective literacy, and less misinformation all decrease perceived risk. Notably, the effect of misinformation is greater for those with lower objective knowledge than for those with greater objective knowledge (Table 4). The interactions of subjective literacy and objective knowledge and subjective literacy and net uncertainty are marginally significant, but the 3-way interaction is not significant (Table 3). This pattern is again consistent with Hypotheses 1 and 2a but not with Hypothesis 2b.
Attitude
The analysis of attitude reveals significant main effects of objective knowledge, subjective literacy, and net uncertainty. None of the 2-way interactions is significant but the 3-way interaction is marginally significant (Table 3). The three main effects reflect the positive effect on attitude of increased knowledge, subjective literacy, and net uncertainty. The marginally significant interaction primarily reflects a greater effect of net uncertainty on those with low objective knowledge, further moderated by smaller differences in the effect of subjective literacy (Table 4). As hypothesized, when respondents have low objective knowledge, the effect of subjective literacy is greater for those with high net uncertainty than those with higher levels of misinformation. However, for those with high objective knowledge, higher subjective literacy has a smaller effect for respondents with higher net uncertainty compared to those with low net uncertainty, contrary to Hypothesis 2b.
Behavioral outcome variables
Two behavioral variables were included—the number of vaccinations received and willingness to recommend vaccination. Willingness to recommend vaccination was associated with significant effects of objective knowledge, subjective literacy, and net uncertainty. Significant interactions were seen of objective knowledge and subjective literacy (marginal), objective knowledge and net uncertainty, and the 3-way interaction of objective knowledge, subjective literacy, and net uncertainty (Table 3). For those with high objective knowledge, regardless of net uncertainty, higher subjective literacy led to greater willingness to recommend. This was also the case for those with low objective knowledge and high net uncertainty. For those with low objective knowledge and low net uncertainty (i.e., misinformed), higher subjective literacy did not increase willingness to recommend and actually decreased it slightly (see Fig. 2). These results are consistent with both Hypotheses 1 and 2.
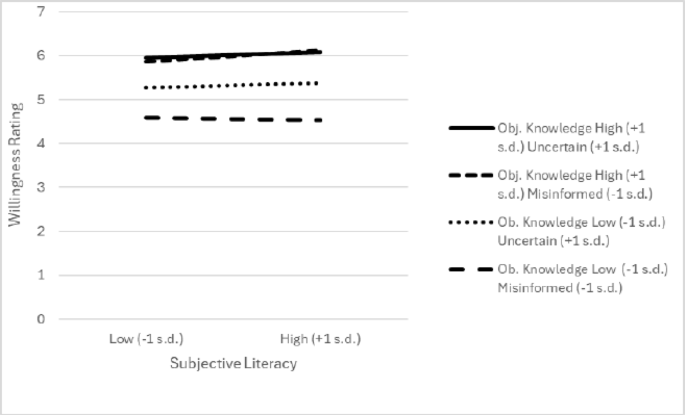
Objective knowledge/uncertainty and subjective literacy effects on willingness to recommend vaccination.
The pattern is similar for number of vaccinations received. Significant main effects of objective knowledge and subjective literacy, and a marginally significant effect of net uncertainty were seen. The interaction of objective knowledge and subjective literacy was significant, and the 3-way interaction approached significance. As was the case for willingness to recommend, higher subjective literacy had a much smaller effect for those with low objective knowledge and low net uncertainty (i.e., misinformed) than for those with high objective knowledge or low objective knowledge and high net uncertainty.