

Fourteen community mental health team professionals in the West Midlands region of England were recruited before saturation was achieved. Participants reported between 1 and 23 years of experience providing LAI antipsychotic care (mean = 9.5 years). 11 worked in Early Intervention and 3 worked in longer term ‘Recovery’ teams [27]. One current recovery nurse had also worked in Early Intervention previously. Twelve had a nursing background although one of these primarily worked as a practitioner in cognitive behavioral therapy for psychosis practitioner now. Two were occupational therapists.
Thematic analysis
Table 2 outlines the results of the thematic analysis.
Non-engagement with LAI in the communityWhat causes LAI non-engagement?
Participants reported that forgetfulness and symptoms of chronic psychosis combine with adverse effects and anxiety to lead to non-engagement. Non-attendance was primarily attributed to forgetfulness rather than strongly held preferences. Forgetfulness was linked to lifestyle factors such as a lack of routine: “some patients can be quite disorganized, lack time, normal structure and routine to their daily lives that they may miss appointments” (interview 2). Participants emphasized how patients gave mundane reasons for missing treatment: “it might be ‘I’m busy’. It might be ‘I have no funds to get there’. It might be that they’re away on that given day” (interview 11). One participant suggested patients may not attend appointments “if they’re not morning people” (interview 14).
Symptoms of chronic psychosis such as lack of insight – “patients don’t believe they have a mental illness so they don’t see the need” (interview 7) – or auditory hallucinations may make attendance difficult: “Yesterday he just slept in because the voices were bad and it was a bit too much for him.” (interview 6).
Patients may miss injections because “Sometimes they’re scared of it” (interview 8) or because of concerns about adverse effects (interview 3) but often give a different “excuse” (interview 9), which makes the exact interplay of forgetfulness, symptomatology, anxiety and adverse effects difficult to establish.
How do professionals currently promote LAI engagement?
Existing approaches to overcoming non-adherence included persuasion, prompting, formal policies, and linking the injection routine with positive experiences. Participants emphasized that these different features all worked together.
Persuading patients to accept LAI antipsychotics was described as “psychoeducation around the benefits of the medication” (interview 1), “providing information about the benefits” (interview 4) and “thinking about how they presented before and how having this medication is going to prevent that” (interview 13).
Practitioners also “prompt” them (interview 8) and help them remember appointments:
We usually find people who are just not that organized writing it on their calendar. Or putting it in their phones. We tend to do text message or phone call reminders. Maybe the day before even, with some people. (interview 3)
Help with travel to the clinic included offering free bus passes or asking supportive relatives to drive patients. LAIs are often delivered in the patient’s home because it is “considerate” (interview 14). However, this makes it more difficult to ensure equipment sterility and privacy and is resource-intensive for the service: “going to their homes… it’s time consuming, it’s draining for yourself and I suppose it’s staff resources as well of having to going out to the person… lots of energy, lots of time.” (interview 4).
‘Road to Recovery’ groups were cited as helping patients gain confidence about leaving the house and participants similarly reported providing informal “graded exposure” to build confidence (interview 14) [28]. Regularly monitoring side-effects also ensured that professionals are alert to the need to switch to a different LAI: “We do try and change medications, especially when people are coming in and we can see that they’re gaining weight, that they’re perhaps kind of feeling more tired. So we do use the LUNSERS to monitor side effects.” (interview 3).
Other participants talked about the ways they helped patients look forward to the day they received their LAI by linking it with positive experiences. Some patients make their LAI into a day out – “quite a lot that will go into town after” (interview 6) – and other professionals members talked about “bargaining” (interview 9) and “bribing” patients to persuade them to accept their LAI:
You’d call it, like, a bribe because we could collect, like, petty cash expenses … We can go get something to eat. We’ll buy you a sandwich. We’ll buy you a cake and a coffee. Something like that. … you sort of go in with whatever you can to sort of engage that person to spend a bit more time with you, so at least you can chat to them and have that time to maybe convince them to have the depot. (interview 10)
Baseline attitudes towards financial incentivesHow did professionals view financial incentives for LAI engagement?
At baseline, support for financial incentives was rated out of 10. The median reported score was 5 out of 10 with participants commenting “I would need to know more about the research” and “I could see advantages and disadvantages of it”. Baseline support ranged from 3 out of 10 to 10 out of 10. All professionals discussed positives and negatives of a financial incentive program, weighing and comparing them.
What advantages of financial incentives were identified at baseline?
Financial incentives were predicted to increase engagement with medication, improving patients’ mental health, and save the service money. A professional who rated their baseline support at 3 out of 10 nevertheless acknowledged “I’ve got a couple of people on my caseload who refuse medication, become unwell, and probably would be open to that idea and it would actually keep them well” (interview 12). Financial incentives could however overcome disorganization-driven engagement “for the people who are just a bit forgetful … It might make people be a bit more regular, prioritize it, you know”. (interview 8).
The priority for the goals of treatment was to avoid relapse which clinicians saw as important for the patient and the health service: “that’s going to be a massive cost to their own health and to society”. (interview 6) The immediate costs of missed appointments were seen as problematic: “if they don’t attend, it’s a massive waste of staff time” (interview 1). The direct benefits of cash were noted as “something to look forward to” (interview 13) and “extra money to help with the kids.” (interview 2).
What concerns about financial incentives were raised at baseline?
Concerns related to patient attitudes to treatment, ethics, and practicalities.
There were worries that financial incentives would not “build the therapeutic relationship” (interview 12). Worse, participants could be “angered if they genuinely can’t make the appointment and then they feel like they’ve lost their £20” (interview 8). Others argued “straight away it’d go on drugs” (interview 10) and suggested that the extra money would lead to worsening mental health “There will be a percentage where the mental health deteriorates because they’re then going to go and use more substances”. (interview 11)
Ethical concerns were raised about “coercive” power dynamics (interview 12) or “bribery” (interview 3). The nuances of consent were discussed:
I feel like it should still be a choice and it is a choice but then you’ve got those vulnerable patients who would jump at that chance (to receive money). (interview 13)
There were fears that the public might consider incentives wasteful, asking “where does the funding come from? … is it coming out of the taxpayers’ money?” (interview 4).
Practical questions relating to implementation included, “how do you keep the money safe?” (interview 6), wondering how long the incentive would last for and whether it would be consistent across different services where LAIs are given, including primary care services (interview 3).
Others were concerned about perverse effects if patients disengage in order to become eligible for an incentive (interview 7) or disengage following incentive cessation (interview 14). One participant raised a contrasting concern: “no one’s ever going to want to come off the depot” (interview 2).
Perspectives after the research presentationDid overall support change?
After a presentation describing the existing research, participants had chance to discuss the research and were asked a second time to rate their own support of out of 10. The new median support was 6.75 out of 10 (range 4–10). Mean support increased by 1.1 out of 10 (range 0–3). One participant who was largely skeptical about incentives reported a score of 4 but emphasized openness to the approach: “if I was informed it was something we were gonna start doing I wouldn’t be entirely against it and questioning my job” (interview 12).
Which evidence did participants’ find persuasive?
The most persuasive data suggested incentives led to increased LAI engagement during the intervention, stronger therapeutic relationships and low levels of substance abuse. Compliance was linked with improved outcomes: “because they were on the depot they were feeling a bit better, and maybe their recovery then improved, and then they were more well, and then able to engage better” (interview 14). Another put it this way:
Using that opportunity to get the depot to continue to build on that relationship and to encourage further engagement and other therapies or interventions that we do, it’s a, it’s a foot in the door. (interview 2)
The size of the cost of the incentive was considered “small change” (interview 4) and “tiny” (interview 6) compared to the cost of LAI treatment. One commented, “It’s a bargain!” (interview 8).
Incentives were conceptualized as rewards and that patients were “being rewarded for taking it, ‘celebrated’ even, that was the word, wasn’t it? And that that was probably a nice way of kind of seeing it” (interview 4).
When I was a child I had my vaccinations. And then after you would get a lolly and a sticker and you know, different things because then it wasn’t as bad. (interview 7)
What ongoing challenges did professionals anticipate?
Ethical and political issues were discussed, but practical challenges were considered in greater detail, several offering potential solutions.
After discharge from mental health services, many patients continue LAIA treatment under primary care teams, leading several participants to wonder whether engagement would decrease if primary care was unable to offer incentives (interview 1). Discharging patients to primary care is a point where patients were seen to disengage from LAI treatment and suggested that if incentives for LAIs continued in primary care then the change might be better tolerated by patients (interview 3).
There was added concern about how to handle cash “safely” (interview 6) and suggesting that a “prepaid voucher” would be more appropriate (interview 2). While some feared that incentives would not be effective, others were concerned that it would be harder to persuade patients to stop LAI treatment, despite acknowledging that services have not previously had difficulty persuading patients to cease LAI treatment (interview 3).
Two participants spontaneously commented that they thought more research was needed. When asked about what would persuade them and their colleagues, participants commented on cost-effectiveness – “how much it would actually improve like the NHS, improve services, cut costs?” (interview 13) – and ensuring research was applicable to their own local population.
Ethical concerns were reiterated more strongly after the presentation. One participant objected that incentives threaten informed consent: “We need to gain informed consent from an individual when we give this medication” (interview 11).
Equity and fairness of incentives were discussed, as it was seen as being unfair on those with good engagement if only those who engage poorly received incentives (interview 13). Another said that “politics” would be a problem (interview 6): “they’re getting more money, they’re already on benefits, all that kind of rhetoric that goes on and on and on really.” (interview 6).
What results did professionals misunderstand?
After the informational presentation covered eight new topics, some participants had misunderstood one of them and we immediately corrected these misunderstandings. Some appeared to have initially misunderstood the finding related to effect persistence after removal of the incentive: “even though the cash incentives stop, people are more likely to continue with their depot” (interview 1) when in fact, following cessation of incentives, engagement returned to baseline and was no different from the control group.
Participants emphasized the finding that LAIA engagement increased but also extrapolated that this would reduce relapses: “We’ll have more people on more antipsychotics, and would have less relapses.” (interview 6) The putative reduction in relapses was linked to wider health system finances: “if it negates one one-month hospital admission, then it’s probably become extremely cost effective” (interview 12).
There was skepticism about the research finding that few study participants spent the money on drugs and alcohol, especially raising the methodological concern that drugs and alcohol use is a “hard one to measure” (interview 11). Another raised concerns that sample sizes in existing studies had been too small to show an increase in LAIA adherence, although in fact a statistically significant result had been found (interview 1).
Comparison with systematic review
Professionals raised 29 of the 40 topics in a recent systematic review [20]. Fig. 1 shows which topics were touched upon before and after the information presentation.
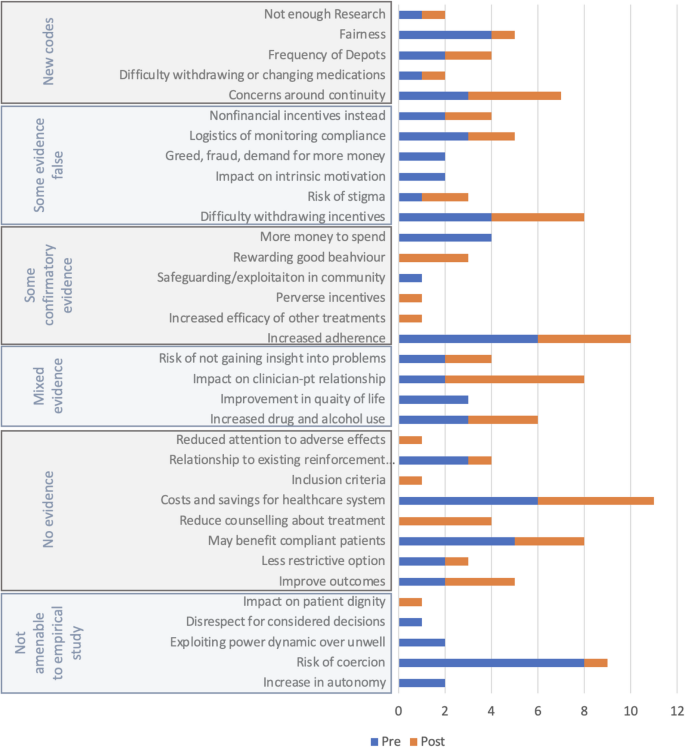
How many participants mentioned each theme from the systematic review before and after information presentations?
Five new themes were identified which had not been identified in the systematic review (Concerns around continuity; Difficulty withdrawing or changing medication; Frequency of LAIAs; Fairness; and, Not enough research). 11 themes from the systematic review were not mentioned in any interviews: flexibility, appropriate incentive size, personalization, increased demand for psychopharmacology, penalizes adherence, sense of entitlement, habit formation, financial dependence, may not work, may not help forgetful people, supplants social support.
Although the idea of unfairness emerged, none specifically suggested that good adherence was penalized. Participants also suggested patients taking LAIs would not wish to stop taking their LAI, but no participants said overall demand for antipsychotics would increase.
Figure 1 shows that in the pre-information interviews, participants brought up topics which were rated ‘not amenable to empirical study’ in the systematic review, such as the idea incentives increase autonomy or may be coercive. After the information session they prioritized practical issues like continuity and the withdrawal of incentives, the importance of increasing adherence, therapeutic relationships, and health economics.