Data: CDC (https://www.cdc.gov/overdose-prevention/data-research/facts-stats/opioid-dispensing-rate-maps.html)
Tool: Mapchart (https://www.mapchart.net/usa.html)
Posted by snakkerdudaniel

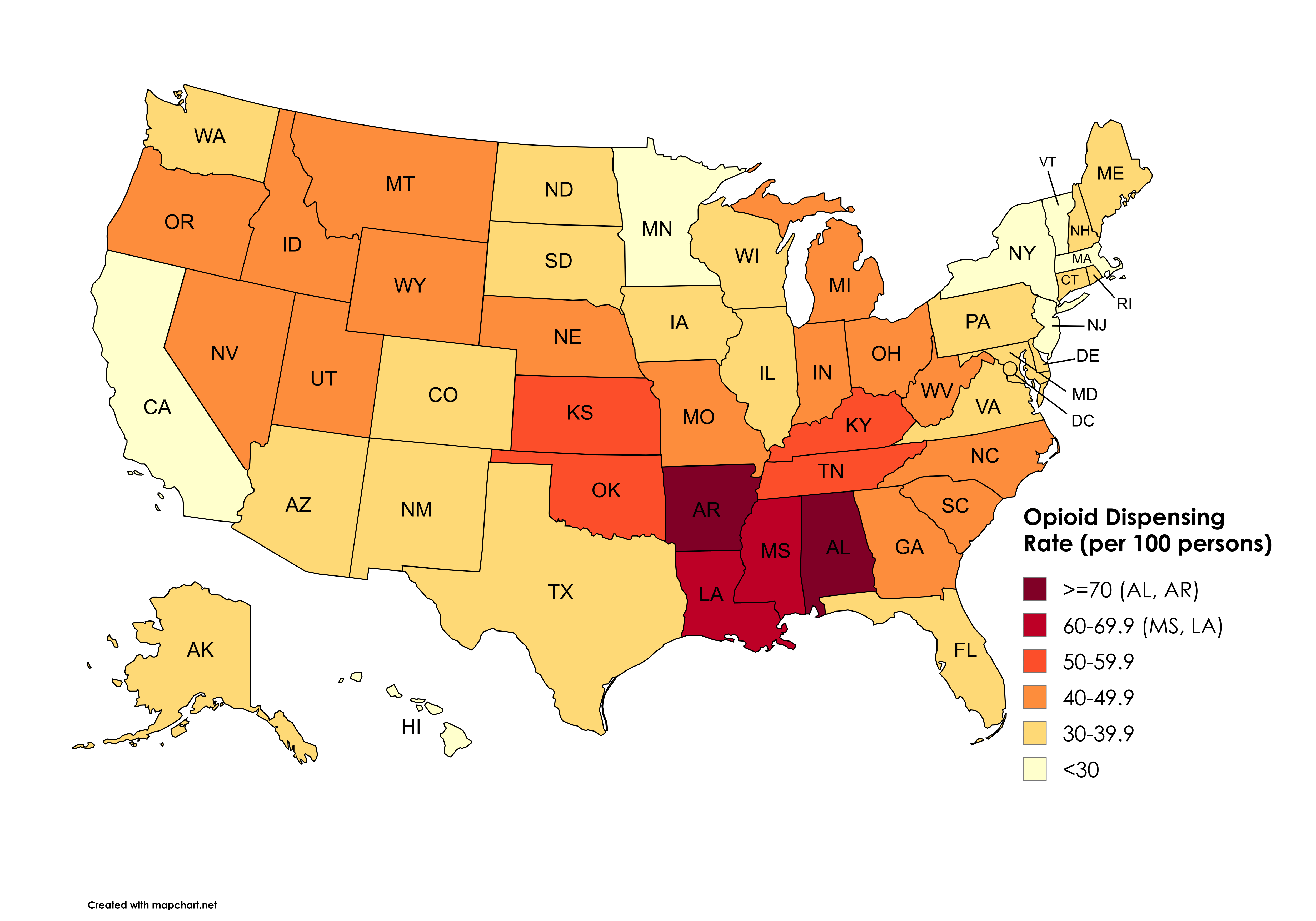
![[OC] Opioid Dispensing Rate (per 100 persons) by US State in 2023](https://www.byteseu.com/wp-content/uploads/2025/09/cm1fuiub9fpf1-1536x1075.png "[OC] Opioid Dispensing Rate (per 100 persons) by US State in 2023")
Data: CDC (https://www.cdc.gov/overdose-prevention/data-research/facts-stats/opioid-dispensing-rate-maps.html)
Tool: Mapchart (https://www.mapchart.net/usa.html)
Posted by snakkerdudaniel
16 Comments
What is a dispensing rate?
My poor Louisiana, riddle with opiates and chlamydia.
I have to be misunderstanding this. Nearly the entire country has opioids prescribed at greater than 30 people of 100? Some places have greater than 70% of people being prescribed opiods? How is that possible?
Mississippi come on! You know you are better than your neighbors! Look at how well you have been doing in these on Reddit recently!
Minnesota always crushing it
Keep up the good work
As an ex-pharmacist in the UK, I’m stunned that it’s per 100 persons.
I looked, thinking that it was per 1000, and thought ‘higher than I’d expect’.
That’s an unbelievable figure.
Overlay this with obesity rates
If I had to wake up in Arkansas everyday, I’d need some shit too.
I was in disbelief at first but when I thought about it, I realized that I had a prescription for pain after a kidney stone surgery and then also some cough syrup I have probably has some in it, too. You’d have to bring in a few more dimensions like frequency and type to really get an accurate idea of where abuse might be occurring.
I’m an RN in Arkansas and not surprised at all, the older generations are absolutely zonked out of their minds all day on opiods, muscle relaxers, and benzos. They are absolutely addicted to these medications and will move and harass their PCPs endlessly for more.
These maps never surprise me…
Oh goody, yet ANOTHER “different colored states” map.
I just finished reading “Death in Mud Lick, A Coal Country Fight Against the Drug Companies that Delivered the Opioid Epidemic” by Eric Eyre. Data like this is only available because a LOT of dedicated people have fought against the people who have tried to keep these numbers secret. They were delivering hundreds of thousands of pills a month to pharmacies in towns with a a few hundred people. Some of the damn pharmacies had little concession stands set up to deal with the line ups of people.
This is good information but I’ll caution that the opioid dispensing rates is increasing in some places because we’re asking prescribers to write for shorter courses post-injury or post-surgery (e.g. 3 days) and e-prescribe additional short courses when needed. That leaves fewer unused pills in the community, but increases the number of dispensing events.
I used to provide academic detailing to physicians with their opioid prescribing data, compared to benchmarks and their peers. We had to ensure they understood that we wanted lower milligrams and fewer pills, not necessarily fewer prescriptions.
Trying to decide if this is a data sub or a shit on the south sub
Oh wait – this is a political spambot account, isn’t it?