

Diagnosing endometriosis has traditionally been a slow and difficult process. In the United States and the United Kingdom, clinical guidance now acknowledges that relying solely on surgery to confirm the condition has contributed to long delays, often spanning many years. To improve this, clinicians are now encouraged to suspect and manage endometriosis based on an individual’s symptoms, medical history, and imaging, rather than delaying care until it’s confirmed by invasive laparoscopic surgery.
Endometriosis is a chronic, progressive condition where tissue similar to the lining of the uterus grows outside of it—often forming patches of tissue (known as lesions) on the ovaries, fallopian tubes, and the lining of the pelvis. These lesions respond to hormonal changes that can lead to inflammation, pain, and scarring.
Public awareness has grown in recent years, helped by celebrities speaking openly about their experiences. Comedian Amy Schumer, for example, described endometriosis as “a lonely, lonely disease” and shared that doctors removed 30 lesions and her appendix during surgery—highlighting how severe the condition can be despite being invisible from the outside.
The increase in awareness and changes to clinical practice coincide with efforts from patient advocacy groups, the scientific community, and government agencies to better understand what is happening inside the body. For example, in 2024, the National Institutes of Health launched the RADx® Tech ACT ENDO Challenge to accelerate the development of non-invasive diagnostic tools for endometriosis.
Researchers now recognize that endometriosis is an estrogen-dependent, chronic, whole-body inflammatory condition—not just tissue growing where it shouldn’t. It is characterized by elevated inflammatory markers, which can fluctuate with the menstrual cycle. Unlike many other inflammatory diseases, this inflammation is closely linked to hormonal activity, impacting the timing and severity of symptoms.
New technologies—especially proteomics, the study of proteins—are helping scientists uncover the biological processes driving the disease and its symptoms. These insights could help speed up diagnosis and lead to more targeted treatment options.
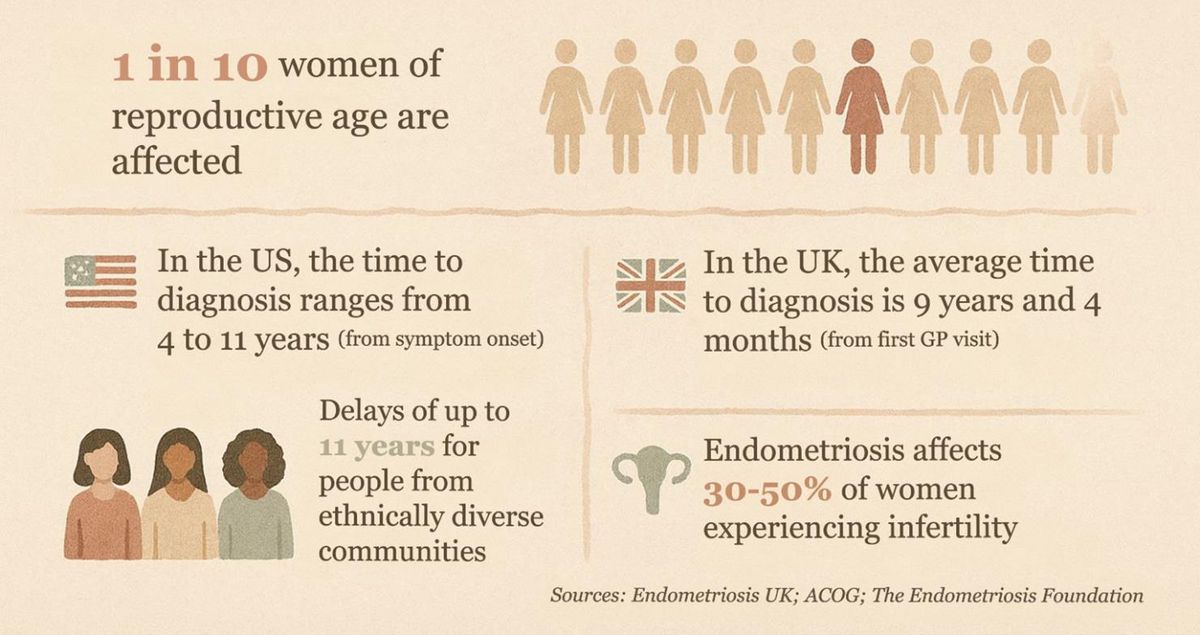
Figure 1: Endometriosis facts and figures. Credit: AI-generated image created using Microsoft Copilot (2026).
Why is diagnosing endometriosis so difficult?
Endometriosis doesn’t look the same for everyone. Symptoms can include severe bloating, painful periods, pelvic pain, pain during or after sexual intercourse, bowel or bladder symptoms, fatigue, and fertility challenges—many of which overlap with other conditions.
Associate Professor Sarah Holdsworth-Carson, research manager at the Moyna Fox Fertility Research Centre, focuses on improving the diagnosis and classification of endometriosis through translational research that connects laboratory findings with patient care.
“There are so many symptoms linked to endometriosis, and people with the condition can have a combination of these symptoms or be completely asymptomatic… Education at the community and medical level is critical to improving recognition,” she explained.
Like many, she has lived experience of the condition but was fortunate to receive an early diagnosis at the age of 19, during her undergraduate degree. This, she notes, strongly influenced her decision to pursue research in women’s health.
“As my knowledge about endometriosis grew, I became fascinated by the heterogeneity of the condition, both at the symptom level and the appearance of lesions,” she added.
The wide range of symptoms—combined with social stigma—explains why diagnosis is typically delayed. “As a society, we are not very good at talking to peers, family, or health professionals about menstrual health and painful periods or intercourse. There is a normalization of pain associated with menstruation, and many people do not seek help,” she said.
Findings from an online survey of > 3,000 people diagnosed with endometriosis, conducted by Endometriosis UK, showed that, on average, it took 3.5 years from first noticing symptoms to seeking medical help. Even then, many did not feel heard: 83% of respondents reported being told their symptoms were normal, that they were “making a fuss about nothing”, or experienced similar dismissal from a healthcare professional.
In a social media video intended to raise awareness and encourage others to seek help, Schumer said: “You know, for months, I had been complaining of pain…it was just this pain you can’t see. And, you know, there is the inclination to always think a woman is just being dramatic. We have to advocate for ourselves; we have to speak up.”
When you combine repeated dismissive experiences with the vast array of physical symptoms, it’s understandable that mental health can suffer. A large study from Yale School of Medicine, analyzing > 8,200 individuals with endometriosis and 194,000 controls, found significantly higher rates of depression, anxiety, and eating disorders among those with the condition.
“Early detection and therefore more timely treatment of endometriosis could theoretically reduce the risk of developing chronic pain symptoms and infertility,” emphasized Holdsworth‑Carson.
What biology is revealing about the disease
Although the exact cause of endometriosis remains unknown, scientists have identified several key processes that help explain why the disease persists and causes pain. These include chronic inflammation, immune system changes, new blood vessel growth (angiogenesis), and nerve growth.
“Immune dysregulation is likely responsible for the establishment and progression of lesions, and the resulting inflammatory environment,” said Holdsworth-Carson. Endometriosis involves both the innate immune system and the adaptive immune system. Innate immune activity promotes an inflammatory environment, while adaptive immune dysfunction reduces the body’s ability to clear abnormal cells.
“There are many unanswered questions… but a focus on the heterogeneity of endometriosis lesions is needed to develop more meaningful disease stratification and personalized treatment options,” she added.
Different lesion types (i.e., superficial, deep infiltrating, ovarian) show distinct biology and behavior, with differences in molecular profiles, depth of invasion, and related symptoms.
The role of angiogenesis in endometriosis
Endometriotic lesions require a blood supply to survive. Angiogenesis—the formation of new blood vessels—is normally tightly regulated by a balance between pro-angiogenic and anti-angiogenic signals. In endometriosis, excess pro-angiogenic signals, particularly via vascular endothelial growth factor (VEGF) signaling, trigger the sprouting of new vessels. This provides oxygen and nutrients to lesions, allowing them to establish and grow outside the uterus.
“Angiogenesis plays an essential role in the growth and survival of endometriotic lesions in endometriosis,” explained Professor Ronald Wang, division head of the Department of Obstetrics & Gynaecology at The Chinese University of Hong Kong. Wang’s research focuses on reproduction and development.
Lymphatic vessels also play a role, facilitating the spread of endometrial cells and supporting immune cell trafficking, which, together, contribute to the chronic inflammatory environment. This process is closely linked to immune dysregulation. Pro-inflammatory cytokines stimulate the production of vascular growth factors, creating a feedback loop that sustains inflammation and lesion growth.
Many of the proteins involved in these pathways—including VEGF family members—are measurable in biological fluids, making them attractive candidates for proteomics-based diagnostics.
One key molecule is vascular endothelial growth factor C (VEGF-C), which is elevated in ectopic endometrial tissue. VEGF-C promotes endothelial cell activity, increases vascular permeability, and supports both angiogenesis and lymphangiogenesis—the formation of new lymphatic vessels.
As Wang explains, “because VEGF-C is involved in disease progression, it holds promise as a potential biomarker and therapeutic target. Detecting or modulating this pathway could open new avenues for both diagnosis and treatment.”
“Our studies suggested VEGF-C as a potential biomarker of angiogenesis and a target of anti-angiogenesis therapy for endometriosis. How specifically and sensitively VEGF-C can be detected by biochemical, molecular, or imaging methods—and how it can be targeted by new or existing pharmaceuticals for diagnosis and treatment of endometriosis—may require further studies,” said Wang.
Biomarkers like VEGF-C can be measured using techniques such as enzyme-linked immunosorbent assay and liquid chromatography–mass spectrometry (MS). Emerging approaches, including AI-assisted drug discovery, may also help identify promising therapies that can target angiogenesis pathways.
Why we still don’t have a reliable blood test
Despite decades of research, there is currently no widely approved, clinically validated biomarker test that can definitively diagnose endometriosis on its own. Blood tests that focus on cancer antigen 125 (a protein sometimes elevated in endometriosis) can be measured, but they’re not specific or sensitive enough to diagnose or rule out disease by themselves, and levels can be elevated by other conditions, such as ovarian cancer.
Some countries are exploring alternative diagnostic tools; for example, researchers in France have developed a saliva‑based test, which has been supported by the French government.
A lot of Holdsworth-Carson’s research had originally focused on the genomics/transcriptomics of endometriosis, and as she puts it, “frustratingly, these avenues don’t really reflect the dynamic nature of the disease, whereas a large‑scale proteomics approach gives a real‑time functional snapshot.”
Proteomic studies can identify hundreds of proteins that differ between people with and without endometriosis. One study, involving Wang, used proteomic profiling to reveal diverse protein patterns across clinical samples. By systemically integrating and analyzing these data, it highlighted potential biomarkers that could support earlier, non-invasive diagnosis and offered insights into novel therapeutic targets.
A promising step toward non-invasive diagnostics came from researchers at the University of Melbourne and the Royal Women’s Hospital, in collaboration with Proteomics International Laboratories. Using a proteomics workflow, the team analyzed plasma samples to identify and validate protein biomarkers associated with endometriosis. This approach goes beyond single-marker testing by capturing a broader snapshot of disease biology.
Speaking about the development of this blood test —the Promarker®Endo—which utilizes precision MS technology, Holdsworth-Carson explained: “I was interested in two factors: 1) non-invasively diagnosing endometriosis, avoiding the need for invasive or intimate procedures (such as surgery and vaginal ultrasound), which a routine blood test could offer, and 2) applying a technology that better illustrates the real-time functional snapshot of disease mechanisms, progression and differences relevant to disease changes and treatment response, which a large-scale proteomics approach could do.”
She emphasized that endometriotic lesions are highly heterogeneous and dynamic, with appearances changing over time, and that intra-individual variation adds complexity: “A biomarker for endometriosis would need to accommodate these potential differences. As proteomics can capture real-time biological state, this approach [PromarkerEndo] holds a lot of promise.”
The study, which involved Holdsworth-Carson, demonstrated that panels of circulating proteins could distinguish individuals with endometriosis from those without it.
Wang noted: “Proteomics is good to provide functional insights, discover biomarkers, and more direct clinical applications”, but cautioned that it also “has a wide dynamic analytical range leading to high detection variability.”
Because endometriosis is so heterogeneous, combining proteins, genes, and metabolites—known as multiomics—may reveal a clearer picture.
Three goals for the future
Holdsworth‑Carson outlined three key goals for the future application of proteomics in endometriosis:
- Better classification of the disease: akin to molecular staging in breast cancer, allowing individuals to receive tailored treatment.
- Routine monitoring: capturing how the disease changes over time using non-invasive tests—such as blood, urine, or other bodily fluids—so management and treatment can be adjusted based on real-time profiles.
- Integration with multiomics: combining proteomics with other ‘omics technologies and patient-specific clinical data to build a multi-dimensional diagnostic framework.
As proteomics and multiomics methods advance, the hope is that earlier diagnosis, individualized treatment, and better long-term management will become possible.