
We identified 5415 records through the database searches and other methods; after removing duplicates, 3564 remained. After abstract screening, 205 records moved on to the full-text screening. Based on the full texts, we included 40 studies meeting our eligibility criteria (see Fig. 1). We sampled 25 studies for in-depth qualitative synthesis based on data richness28.
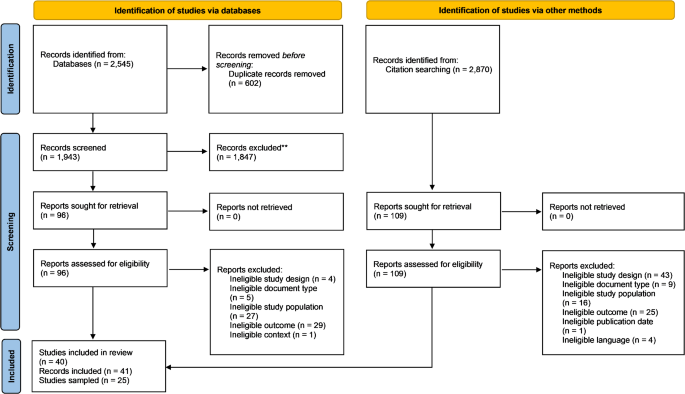
Prisma Flow Diagram according to Page et al.28. This diagram illustrates the process of selecting studies for inclusion in the review. It shows the number of records identified, screened, and included, along with the reasons for exclusions at each stage of the review process.
Study characteristics
Table S8 (Appendix) presents the study design, research methods, research aim, country, setting, and key sample characteristics of all 25 sampled studies. Most sampled studies originated from the US (n = 6), Australia (n = 4), and Finland (n = 2). Six studies29,30,31,32,33, focused exclusively on children (aged 8–14 years), while 15 34,35,36,37,38,39,40,41,42,43,44,45,46,47,48 included adolescents (aged 15–19 years) or both. Three studies37,49,50 did not report specific age ranges. Nineteen studies29,31,32,33,34,35,36,37,38,39,40,41,43,44,45,−46,49,50,51 provided information on sex, with a predominance of females in most studies. Three studies35,37,40 had more male than female participants, and two43,51 reported an equal distribution. One study52 had only male participants. Gender was explicitly addressed in one of the sampled studies47. Twelve sampled studies29,30,31,32,35,36,39,42,43,45,49,50 were conducted studies with children or adolescents with diverse characteristics (e.g., ethnicity, socioeconomic status, disability, illness). Eleven of the included sampled studies29–32,35−37,39,41,45,48–50,52 utilized focus groups. Interviews were employed in six studies29,34,40,44; eight30,33,42,43,45,46,50,51 adopted mixed-method approaches.
Synthesis of findings
We synthesized our analysis findings into a model (see Fig. 2). Following the model from the inside out, the findings are detailed in the following chapter (see Table 1 for findings description and Tables S12 – S13 in the Appendix for the GRADE-CERQual qualitative evidence profile).
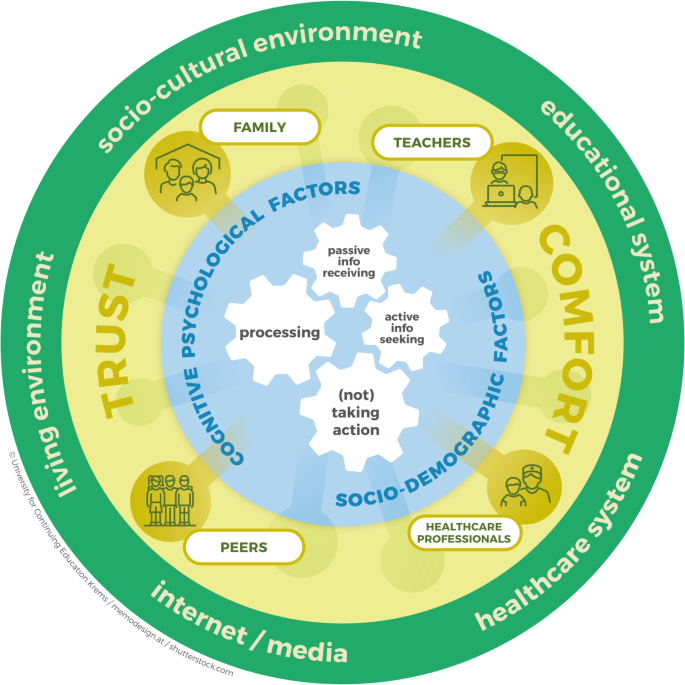
Literature-based model on health literacy from children’s and adolescents’ perspectives. The model is organized around cogwheels at its center, which represent the core components of the health literacy process. The blue area encompasses various individual cognitive, psychological, and sociodemographic factors. Expanding outward, the yellow area illustrates how health literacy is embedded within social relationships. The green circle highlights the socio-cultural environment, including the educational system, healthcare system, internet/media, and living environment.
Finding 1: active information seeking (moderate confidence)
Adolescents usually have a reason to actively seek health-related information40,46,49. Adolescents mentioned that experiencing symptoms prompts them to seek information40 to understand the symptom causes or treatments46 or to learn strategies46,53. They explained that they want to validate or reassure themselves about their symptoms40,46. The following adolescents’ quote illustrates: “I am looking at when to see a doctor to see if it’s a serious thing”40 p. 4. Adolescents stated that they search for health information before or after a health appointment46, or when they forgot to ask a question during a doctor’s visit49.
Adolescents mentioned that they utilize the internet38,45,49 and traditional media (TV, radio)38,42 but also friends, family, and teachers38,42 as health information sources, and that when seeking sensitive health information, they prefer quick, accessible, and complete30 information with personal relevance32, high quality, and privacy32.
Finding 2: passive information receiving (very low confidence)
In several studies, children and adolescents mentioned that they also receive health-related information passively (i.e., without searching)29,39,42,46. Adolescents confirmed that they receive health information from health practitioners39,42, parents, peers, and schools42 , and by learning from family health behavior and others’ and personal experiences29,42.
Finding 3: processing (moderate confidence)
The authors concluded that children and adolescents rely on existing mental frameworks that evolve as they gain new information or experiences. The complexity of their understanding varies based on how involved they are in their own health decisions29,30. Several authors indicated that children and adolescents are conscious of mis- and disinformation and potential health risks39,40,44,46,49. Adolescents reported an awareness of potential disinformation in online sources, and some experienced difficulties evaluating the relevance because of information overload40.
Adolescents exhibited varying levels of trust in health information from celebrities, health professionals, parents, friends, intervention providers or manufacturers34, and social media46. Adolescents reported frustration after not finding needed health information, a reassured feeling when finding others on the internet with similar experiences46, and confusion due to the diversity of statements44. One adolescent reflected that, “In one material, it is written that someone has to drink 8 glasses of water every day. In one other article that you have to drink as much as you want. In another article, that you can’t drink a lot, because it’s harmful. It is confusing”44 p. 10. Adolescents revealed that uncertainty in their health knowledge led to self-doubt in their decision-making processes49.
The steps of processing health information include paying attention, thinking, reflecting, asking questions, and questioning the health information and its reliability44,48. Some adolescents possessed a foundational understanding of health-related research and scientific principles34. Authors revealed that only few actively compared data across multiple sources to verify its validity45 or considered its reliability44. Adolescents in another study mentioned that actively consulting others or finding additional sources to corroborate is a common practice in making health information judgments34. Adolescents in a third study stated that they evaluate the reliability of health-related content using diverse criteria. For official websites, they check elements like URLs, logos, and professional appearance, while on social media, they consider factors as likes, dislikes, and user interactions48.
The authors of one study33 reported that children rated food as good or bad for their health, influenced by their individual experience or knowledge. Some participants in Subramaniam et al.’s45. study described that they rely on others’ appraisals (e.g., teachers, relatives). Adolescents in several studies considered the financial cost of a health product34,36,46 as a quality indicator, believing that a higher investment signified a more reputable product36.
Finding 4: (not) taking action (moderate confidence)
Whether children and adolescents can make informed health decisions also depends on their knowledge and opportunities, including understanding and expressing health-related rights and responsibilities in the healthcare system, as adolescents39 mentioned. According to Massey et al.’s39 and Taba et al.’s studies46, some adolescents considered parents as gatekeepers. Adolescents shared experiences of parents gradually entrusting them with more responsibilities, signaling a transition toward greater autonomy in managing their health39.
Knowledge about health can affect children’s51 and adolescents’44,50 responsibility level51 but is not a guarantee for engagement in behavior50. Adolescents mentioned that, before making a health-related decision, they consult a healthcare provider36 to compare arguments and pros and cons36, and consider near-term consequences41.
In one study, boys described barriers to taking action for mental health issues, including stigma, privacy concerns, and the need to protect themselves or those close to them. Some avoid taking action for their mental health, believing such issues are not aligned with “boy culture,” as illustrated by the following quote: “Yes, but it’s not the coolest thing for a boy to say that I have thoughts or want to commit suicide.”52, p. 6. Furthermore, boys in this study cited a lack of knowledge about mental health and whom to approach as key reasons for not taking action. They felt they needed a strong justification to see a school nurse and were unsure when symptoms became serious enough to seek help52.
Finding 5: cognitive psychological factors (moderate confidence)
Adolescents in four studies31,39,49,50 recognized the role of a future-oriented attitude, personal motivation, self-efficacy, and risk perception as psychological factors influencing the adoption of healthy behavior.
Adolescents mentioned that future-oriented attitudes influence health literacy. While many questioned the need for preventive health visits or the long-term consequences of their current health behaviors49, others expressed positive attitudes toward preventive screenings39. Adolescents’ use of health literacy skills is influenced negatively by low personal motivation and positively by high personal motivation (e.g., because of sports goals)31,49. Adolescents in Parisod et al.’s31 study discussed that individual motives and motivation levels led them to engage or not engage in health-risk behavior. For example, while some smoke cigarettes to be socially accepted, others refrain because of smoking’s negative effect on athletic performance. Chronic illness can also lead to high personal motivation levels, as explained by one adolescent who goes to body checks more often due to illness49. Adolescents emphasized that individual self-efficacy plays an important role in resisting social pressure and making healthier choices31,32. Furthermore, adolescents identified low risk perception as an important determinant, as some perceived certain health issues as not serious, which reduced the use of health literacy skills in decision-making49.
Adolescents and children noted medical terminology as a barrier34,40,45,46. Three studies36,42,45 found that knowledge and skills affect to which degree adolescents can seek health-related information or make informed health decisions. Some children and adolescents stated in these studies that their understanding of health information is significantly influenced by whether they can read and understand the given information or formulate relevant search strategies, as illustrated by one adolescent: “I don’t really know how to spell it [endometriosis]. I saw something about this on television, and I did actually want to know more about it, but I didn’t know how to spell it”36 p. 242.
Finding 6: socio-demographic factors (moderate confidence)
Children and adolescents stated that their gender identity plays a role in the patient–provider relationship37, the gender perceptions children develop relevant to health responsibilities33, and in developing concerns about body image and lack of self-esteem32. Some adolescents in a study conducted in Mexico indicated that interacting with an opposite-gender provider could lead to feelings of embarrassment. The following quote illustrates: “You feel a lot of embarrassment because, they tell you ‘raise your blouse a little bit so I can check your stomach,’ and you say like, thinking ‘oh, no, how embarrassing’”37 p. 8. The children in another study33 showed that the gender-associated roles were clear, as they mainly discussed their mother’s responsibility and role when it came to healthy eating. Adolescent girls in Smart et al.’s study32 expressed concerns about body image and self-esteem, as they faced pressure regarding their appearance, leading to unhealthy eating behaviors. In one study, boys described how assumed gender roles (e.g., that boys do not show emotions) shaped their engagement with mental health practices52.
Age determined whether children or adolescents searched for online information. Adolescents in Loers et al.’s38 study stated that they prefer to search online, especially for relevant and applicable health information. Children, however, relied heavily on conversations with family members, as children in Fairbrother et al.’s study mentioned30. Loers et al.38 acknowledged that finding, understanding, and evaluating health information differed by age, and concluded that this may be because of cognitive development. In Smart et al.’s study (2012)32, older adolescents demonstrated more nuanced descriptions of their learning needs and knowledge, and health claims.
Adolescents with chronic sickle cell disease43 described how their condition affects their understanding of health (e.g., they must closely consider health, illness, and treatment options), how they must develop coping mechanisms to manage pain (e.g., relying on family and peer support, finding distractions, seeking refuge in religion) and, more generally, how their health-related decisions and behaviors are affected (e.g., hiding the chronic disease because of fear of stigma).
Adolescents in Parisod et al.’s study31 mentioned that adolescents’ own health status (e.g., having asthma) influences their attitudes about tobacco use.
Adolescents with migration background in two studies found that language constraints can be a barrier to decisions about health-related information42,45. Adolescents in Richter et al.’s study42 mentioned that it was helpful to have translators at doctor’s appointments and that language barriers influenced their ability to read nutrition labels. They acknowledged the important role of guidance from their social networks, leveraging the experiences and insights of others who shared migration experiences.
The impact that socioeconomic background has on health literacy is illustrated by the children’s descriptions in Velardo and Drummonds study33. Some reported limited access to fresh food options due to financial constraints. They understood that financial limitations made it difficult to maintain a healthy diet.
Finding 7: family, teachers, healthcare professionals, and peers (moderate confidence)Family
Family is a major health information source for children and adolescents and a help in processing it29,30,32,34,35,37,42.
Adolescents stated that they discuss new information with family members and consult parents for help with search strategies, managing severe symptoms, scheduling doctor appointments, and discussing online health information before applying it42,46. Some mentioned that they prefer consulting family first for health information instead of using the internet, doctors37, or asking peers32.
One adolescent expressed: “I would definitely first ask my parents, if they have somehow already heard something about it.”38 p. 7.
Chronically ill adolescents43 mentioned that they discuss symptoms with family, which the authors presumed created a sense of belonging and collective security. Conversely, the authors of this study concluded that adolescents do not discuss long-term consequences with their parents, and instead expressed concerns that their condition worries their parents.
Smart et al.32 concluded that trust, comfort, and respect are important. Early adolescents in Parisod’s study31 mentioned that they make observations about their parents and have discussions with them.
Teachers
Several studies reported that children and adolescents access health information from their teachers and consider them a health information source29,31,32,34,35,41.
When counterchecking new health information, many adolescents ask adults, including teachers, as mentioned in Smart et al.’s study32. Adolescents more precisely described needing a comfortable, trusting, and respectful relationship with teachers to discuss health issues with them. Some adolescents in this study mentioned that they do not trust teachers with sensitive health information. Others said some teachers are trustworthy.
Children primarily depended on health classes and teachers among other important health information sources29, despite limited use of the internet and print sources29. For most adolescents, teachers and coaches play roles in disseminating valuable information34.
Healthcare professionals
In some studies, adolescents reported that healthcare professionals are a main health information source29,34,37. Adolescents in Smart et al.’s32 and Taba et al.’s studies46 reported asking doctors to countercheck new health information. Schönbächler-Marcar et al.’s study43 showed that adolescents value expert consultations on medicine intake.
In two studies, adolescents expressed discomfort in gender-specific scenarios and preferred same-gender doctors37,39. The participants in Hoffman et al.’s study37 reported that a lack of doctors’ professionalism and positive attitude was a barrier to a good patient–provider relationship.
Some adolescents appreciated health professionals’ supportive role. Some acknowledged that making an appointment with a primary care physician is a crucial step and that primary care physicians are gateways to the healthcare system (e.g., to specialists)39. Some faced difficulties scheduling appointments at convenient times, while others expressed frustration with long wait times.
Adolescents expressed a desire for continuity of care with the same healthcare provider to mitigate embarrassment, taking to confiding in a “doctor friend”39. Boys in one study expressed that they would feel more comfortable seeking help if they saw their school nurse more frequently, allowing them to build a better relationship52.
Several studys32,34,37,40 showed that trust and comfort level is important for the patient–provider relationship. Adolescents in Taba et al.’s46 study noted trusting health care professionals because “They’ve studied for a lot longer and helped more people than Google”46 p. 9. Doctors’ lack of professionalism has been identified by adolescents as a barrier37.
Peers
Children and adolescents reported obtaining health information from their peers and friends35,38, engaging in discussions about chronic disease43 and health information32, and observing their behaviors31. Children and adolescents reported obtaining health information from their peers and friends35,38, engaging in discussions about chronic disease43 and health information32, and observing their behaviors31.
However, in some studies, adolescents showed that when applying search strategies to access health information, they rarely seek help from peers and, instead, consult their parents32,46. However, in some studies, adolescents showed that when applying search strategies to access health information, they rarely seek help from peers and, instead, consult their parents32,46.
Finding 8: living environment (low confidence)
Eight studies illuminated the influence of living environments on health literacy29,31,33,34,35,45,46,51. Children in Parisod et al.’s study31 emphasized their sensitivity to their surroundings, particularly expressing concerns about the environmental impact of snus litter, which is expressed in a negative attitude toward snus in general. Children in Velardo and Drummonds study33 underscored the significant impact of school canteens on food choices, revealing a preference for unhealthy snacks due to limited healthy options. Children and adolescents drew conclusions from their surroundings, highlighting environments should offer sports equipment and engaging activities, access to valid information to enhance health literacy29,34,45,51, and school interventions to support their practical application of health topics33,34,46,51.
Finding 9: socio-cultural environment (very low confidence)
Adolescents’ religion impact their health literacy skills use, leading some to avoid doing something against their religious moral. One adolescent stated: “They do something that is against their religion so they fear to open up about it”49 p. 9. Some adolescents prioritized discussions about mental health over physical, while highlighting the persistent stigma hindering open discussions around mental health topics35.
Richter et al.42 summarized that it is difficult to separate the effects of language barriers, limited social support networks, lack of time, different cultural food practices, and other related factors when it comes to the influence of migration background on health literacy.
Finding 10: educational system (low confidence)
Children and adolescents found that school discussions, materials, and lessons shaped their understanding of health-related matters29,31,32,33,34,49,51. One quote highlights: “School, like when you’re in health class and we learn more about like health stuff”49 p. 8.
Children appreciated programs such as school gardening initiatives that sparked conversations about health within their families, indicating the broader impact of such interventions on their health literacy learning experiences33. Adolescents also recognized the influence of access to school health classes in facilitating their health literacy development49. Furthermore, adolescents mentioned applying media or health literacy49 in seeking online information, and search strategies learned from digital literacy in school or school assignments46. The relationship to their teachers plays a pivotal role.
Finding 11: healthcare system (very low confidence)
Five studies32,37,39,46,49 reported information on the healthcare system and relationship as factors influencing health literacy.
Massey’s research39 revealed that adolescents faced barriers to accessing healthcare services due to discomfort, emphasizing the importance of trust in providers and continuity of care with the same healthcare provider to mitigate embarrassment. Competencies related to health literacy empowered adolescents to overcome barriers, such as difficulties scheduling appointments. Additionally, adolescents recognized the role of primary care physician as gateway to specialized care39,46. Adolescents in one study described social media content as helpful after negative experiences of navigating the health care system or when they do not feel comfortable accessing health system support47 .
Adolescents mentioned the importance of access to healthcare providers and health information in health literacy acquisition. Positive experiences facilitated easy access, poor access hindered the ability to learn about health. One quote highlights: “Not enough clinics around to talk to people and teach them about health”49 p. 8.
Finding 12: internet/media (moderate confidence)
Adolescents relied on digital platforms such as the internet and social media for health-related information32,35,36,38,39,43,46,49. They tended to prefer searching online for relevant information, altering their seeking behavior based on challenges in finding information and situational accessibility38. They actively sought information via search engines and in social media35,36,43,46,49.
Children and adolescents reported that they received health-related information through social marketing campaigns and TV and internet advertisements30,31,49. They considered appearance, quality, relevance, language, style, ranking, country of origin, and source in appraising health information34,38,44,46 and preferred comprehensive, clear, interesting (e.g., in a humorous way)48, and simple information38,46. They acknowledged the importance of structured, balanced health information, mentioning bullet points, keywords, short summaries, and clear and simple explanations with plain language as useful and age-appropriate40. Some prefer information from well-known organizations, such as universities and governments40,45,46 and authors with professional expertise and degrees45,46.
Adolescents understand social media such as TikTok as an easy and free way to access health information and to find support, even if they are aware of the challenges (e.g., algorithms, monetary motivations of content creators, censorship, self-diagnosis)47,53. One adolescent acknowledged that in social media “there’s not a whole lot of pressure to engage with. If you want to learn more or if you want to engage, you can.”47.
Adolescents asserted that one advantage of social media is that they are able to remain anonymous47,48. Adolescents in three studies stated that they find other users lived experiences and opinions on social media platforms helpful, even if they question the reliability of the information provided47,48,53.
Adolescents stated that they view social media platforms like TikTok as a tool to validate and de-stigmatize health challenges. Seeing others share their experiences reassures them they are not alone and offers a chance to connect with supportive online communities47,53. Adolescents with a chronic condition further utilized digital resources to enhance their coping strategies, for example, by accessing social support and exchanging information with others who have been diagnosed with the same condition, sharing symptoms, and providing advice to one another.