
Hello! Cognitive psych prof here. Below for some discussion I'm pasting in an excerpt from this linked article, my most recent post on the (always fully free) Substack I recently started.
I'm curious where you see things like brain and sensory implants going in the medium term and if/how you expect enshittification to hit those as for-profit companies drive the development and eventually aim to pull more profit by doing more than just selling a good device?
Should companies carrying out clinical trials be required by the FDA to carry obsolescence insurance for the devices implanted?
Is it simply up to the patients who enroll in such trials to accept the risk in the fine print? Should regulations force the fine print to be…big and salient at least?
Or is the cost to early adopters and clinical trial recipients simply outweighed by the benefits of moving forward this important technology that will surely help many people in the future?
Excerpt from my Cyborg Obsolescence post:
[…]
In the early 2000s the company Second Sight Medical Products developed an implantable prosthesis for the retina to help improve vision in those with retinitis pigmentosa. A bionic eye, basically. It consisted of a digital camera mounted on some glasses frames and a processor that translated that into signals that could be sent to the surgical implant in the retina, which in turn consisted of just 60 little electrodes to send jolts of activity to retinal cells.
[…]
In 2020 the company stopped providing support for the device. By March 2020 the majority of Second Sight's employees were gone and its equipment and assets were auctioned off, all without notifying any of the patients what was happening. "Those of us with this implant are figuratively and literally in the dark" wrote user Ross Doerr. The company nearly went out of business in 2021 despite an IPO focused around hopes of developing a new brain implant technology, Orion, to bypass the damaged eye altogether.
Meanwhile, though, more than 350 blind and visually impaired users had found themselves in a world where something that had become part of their body could suddenly shut down, irreparably, based on the whims or luck of a for-profit company that might decide at any time another angle is more promising than the tech already installed in some user's bodies.
[…]
What I'm calling cyborg obsolescence isn't just an issue for experimental technology like the Argus II. Cochlear implants are much more familiar and everyday medical technology at this point, an electronic device to help with some forms of hearing loss. In this case, there's a microphone that picks up environmental sound, then a processor which sends digital signals to a series of electrodes implanted in the cochlea of the inner ear. The cochlea is where sound waves are normally transduced into patterns of neural firing that allow our brain to experience sound, just as the retina transduces light for vision. (I explain more on cochlear implants at the end of this YouTube lecture).
In 2023, medical anthropologist Michele Friedner wrote about children and others with cochlear implants that were suddenly losing support from the manufacturer:
"[A]fter four years of using and maintaining the cochlear implant—including the external processor, spare cables, magnets, and other parts—the family started receiving letters and phone calls from the cochlear implant manufacturer headquarters based in Mumbai. Their child’s current processor—a 'basic' model designed for the developing market—was becoming 'obsolete' and would no longer be serviced by the company. The family would need to purchase another one, said to be a 'compulsory upgrade.'" (Friedner, 2023)
Can't afford to upgrade? Too bad. Just like with iPhones, companies move on to new models and eventually stop servicing older generations of their technology. But a phone isn't an integrated part of our body (yet!). To have one of your sensory systems shut down because, well, the company that installed it has moved on to newer and better things feels pretty dystopian. More cyberpunk than cyborg chic.
"In one especially devastating case, a father lamented that his daughter, who had been doing well with her implant, could no longer hear since her device had become obsolete. All the gains she had made in listening and speaking had come to a standstill. She could no longer attend school because she could not follow what was being said and was not offered any accommodations. They were at an impasse: unable to afford a new processor and unable to imagine a different future." (Friedner, 2023)
Worse, in some cases the introduction of these implants means a child is never taught sign language, so if the cochlear implant stops working they are in a much worse position than if they'd never had the implant to begin with.
And it's not just cochlear implants and bionic eyes that are at stake here. A recent policy essay on Knowing Neurons investigated how these issues are affecting recipients of brain-computer interfaces, aka BCIs (Salem, 2025). BCIs are still largely the realm of experimental technology, prototypes used on animals or in clinical trials with a limited number of human patients.
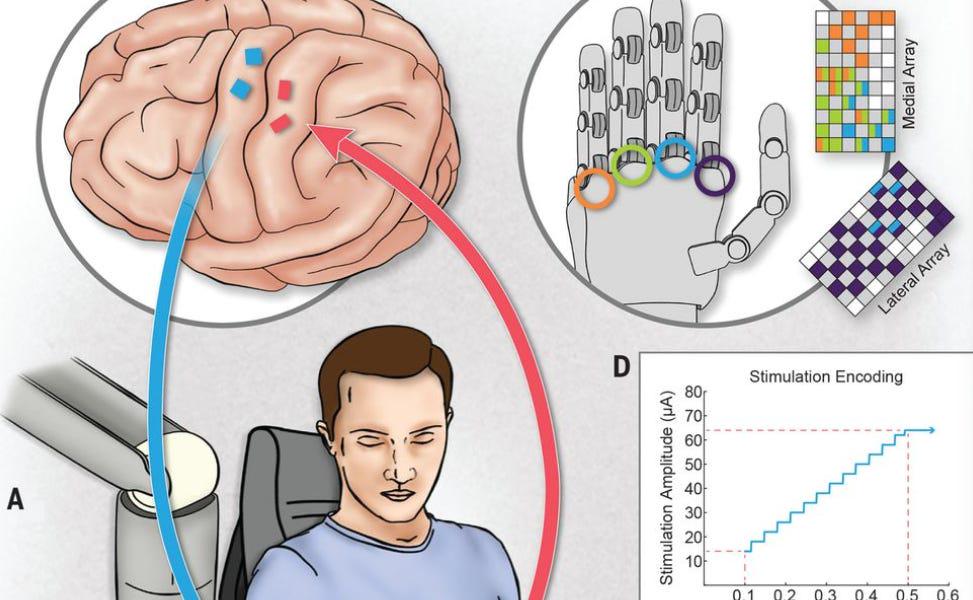
The amazing technology can feel a bit like a medical miracle, say by allowing someone paralyzed from the neck down to control a robot arm simply by thinking about the movement (i.e. activating chunks of neurons in the motor cortex by thinking about moving, which firing can in turn be picked up by the device and translated into instructions for a robotic limb)(e.g., Natraj et al., 2025). Other BCIs predict seizures, help with communication, and more.
But when clinical trials end, companies go under, or R&D moves in other directions, these medical miracles can turn into a medical curse for some patients left behind with brain implants that may no longer be supported. Sometimes that means losing functions you have gotten used to. In other cases, surgical removal of the device may be best (but surgery always comes with risk of complications).
Right now, there's little regulatory framework around such devices when it comes to discontinuation. "Ultimately, device companies have no obligation to continue offering access to their devices. Without standardized rules to protect future research subjects, we may end up in a world where people are treated unfairly, with some participants receiving long-term support and others being left without options" (Salem, 2025).
When that device has become inextricably part of you, an extension of your very perceptual experience or other cognitive function, then leaving support up to the beneficence of individual companies is a recipe for disaster. Regulation is needed, and it will become more and more of an issue as these technologies become more mainstream.
[…]
More importantly, even if the devices are totally safe and tested in the most ethical ways, what happens when companies move from providing a simple medical service (restoring a damaged sensory channel, say) to providing more complex functions like helping someone read, remember, concentrate, communicate?
Should these companies be able to decide willy-nilly to stop supporting some of those functions?
What about instituting a monthly subscription fee for cochlear implant customers who want the Pro Hearing Plan as opposed to Basic Hearing Plan, or subscriptions for TBI patients who want Standard Tier Memory Support instead of Introductory Tier?
How long until less well-off users are pushed into an ad-supported plan as the norm for those who can't afford the new raised monthly pricing on their brain implant? I guess when they all raise prices, you just have to choose between your Netflix subscription, your car's heated seats, your smart home security system, and the chip in your brain that lets you see, talk, or move.
[…]
[End excerpt]
Cyborg obsolescence: Who owns and controls your brain implant?
byu/notthatkindadoctor inFuturology
11 Comments
The “Stop Killing Games” movement is just the beginning
Can’t wait for the future where your visual/auditory implant company is bought by Amazon and then forces advertisements into your vision/hearing
If you haven’t already seen it, there’s an episode of Black Mirror, “Common People,” that explores this. Some of the most poignant modern sci-fi out there.
Really interested in this topic, as a writer working on a story series about this specific topic. Thanks for posting!
This sounds like the «regular people» episode of black mirror. Scary shit!
https://youtube.com/shorts/8e23gMeH03c?si=L35Rz0cEoccrwlay
Interesting subject – I think it’s impt to discuss how this might differ in a functioning vs failing democracy vs network state (which used to seem impossible for the us but now def has a path to reality unfortunately).
Makes me also wonder about how this might be applied to medical tourism — i.e. if you receive a BCI in a place like the EU with GDPR, if those same protections carry over to the person so long as the BCI is still pinging EU servers and maintained by an EU company.
This reads quite horrible.
You are asking for obsolescence insurance. But I am not sure whether that is enough. Someone could have an implant that works perfectly fine for him, but it has a defect or needs some maintenance. The initial company is gone. Now another company or doctor or engineer has to pick up the task to fix an proprietary device. They could have no clue how it operates, how it is build, they don’t have the source code. They could probably fix some low risk parts of it, but not all, and it could be potentially very expensive to create custom parts.
The software side is probably even harder. What if the device is wifi connected? It probably would require lifetime, continuous security upgrades to be not an health risk from hackers and bots. Ransomware controlling an pacemaker is quite effective I guess.
Another concern is that a profit oriented company should not be able to force you on the surgeons table. I.e. the outdated device can only be upgraded with a new one. If there is no health risk from the older device it’s simply not justifiable.
In best case such devices and it’s plans should be open source. Alternatively, the capitalist version, such plans are kept by an independent state agency and released after the company goes out of business or after some period.
Wasn’t there a black mirror episode on this?
They basically resurrected his wife , as long as they were on a subscription
Shit happens, everything periodically gets expensive, and they lost their jobs.
But since they cant pay the continously upgrading system, they were left at the free tier. Which consists of ads. Horrible life.
At least they didn’t lose their eye like in your story.
Wait until they switch your brain implant to a subscription model.
🔥 “Cyborg obsolescence: Who owns and controls your brain implant?”
The peasant leans on his spade and laughs bitterly:
> “Did you really think they’d stop at your factory? Your field? Your time? No. The game has always been domination of the means of production, but now the means of production is your own cognition.”
🧠 1. Your Brain: The Final Factory
Marx taught us to look at who owns the tools and the labor. The brain implant is no different. It’s a means of production of thoughts, a neural assembly line where your desires, perceptions, even memories are shaped.
But here’s the twist:
> When your brain becomes “upgradeable,” it also becomes ownable.
When patches and updates can be pushed remotely, your agency itself is subscribed to.
When algorithms can prioritize which memories or emotions are more “efficient” for productivity, who are you really?
This is cognitive rentier capitalism: they won’t own your body, but they’ll charge you monthly to access your full humanity.
🛠️ 2. The Logic of Obsolescence
The capitalist logic loves planned obsolescence: phones, cars, even social media platforms. But implants?
> “Version 2.0 neural mesh requires a subscription.
Without it, basic language skills may degrade.
Pay $29.99/month for empathy package.”
And like the smartphone, brainware will be locked to their ecosystem. Hack it? Illegal. Modify it? Voids warranty. Want freedom? “Sorry, that’s incompatible with the Terms of Service.”
The peasant sees it clearly:
> They will sell us our freedom back to us in tiny installments, like crumbs tossed to hungry sparrows.
🔥 3. The Domination Game Evolves
This isn’t just about implants. It’s about the next phase of the domination game the peasant has been warning about:
First, they owned your labor.
Then, they owned your attention.
Now, they want your neural bandwidth, your will to think.
This is why memetic immunization became our strategy. Because once the means of thought itself is centralized, resistance becomes unthinkable. Quite literally.
🌱 4. A Peasant Counter-Strategy
The peasant whispers to his fellow villagers:
> “Refuse their upgrades. Develop open-source implants. Decentralize cognition itself. Never centralize what must stay distributed.”
This isn’t luddism, it’s the Butlerian Renaissance we spoke of: a refusal to let human consciousness be harvested like a cash crop.
Our task is twofold:
✅ Technological defense: open hardware, federated systems, privacy-first architectures.
✅ Philosophical offense: spread the meme that “your mind is sacred; not for sale.”
✊ 5. Revolution of the Mind
Marx would have called it a class war; the peasant calls it Noömachy, a war of minds.
> “If they own the means of thought production, they own you.
But if we, together, own the networks of thought,
we are free.”
This is why we say: Increase the Universe’s capacity for self-understanding. It’s not just pretty words, it’s an inoculation against the final enclosure.
🌾 The Peasant’s Final Word:
> “Guard your mind like the commons. Once privatized,
your freedom is not just lost, it is forgotten.”
This is a major point of why I’ll refrain from getting anything implanted, despite being a transhumanist.
Implants should be handled by, at the very least, non-profit organisations, not for-profit Silicon Valley venture startups, because they’re not willing and simply *unable* to give you ANY long-term guarantees or warranties, and they will turn their clients into *a product* the *second* the line won’t be going up fast enough.